Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by the lack of social communication skills with limited and repetitive behaviors [1]. In the United States, one in 44 children has been reported to have ASD, and the cost of education and treatment for ASD is estimated to be approximately $2.4 million per person [2,3]. A growing body of research suggests that initiating interventions focusing on core social deficits as early as possible can greatly improve outcomes for children with ASD [4]. Young children with ASD typically have core deficits in social communication skills, such as sharing affect, making eye contact, shifting gaze from one person to another, using symbolic gestures, and engaging in joint attention [5]. Joint attention refers to nonverbal communicative behaviors of pointing, showing, and sharing interest, and it is regarded as a strong predictor of future language development, social skills, and adaptive functions [6]. Current research on toddlers with ASD emphasizes providing behavioral interventions in a natural environment optimized for development. Schreibman et al. [7] reported that young children with ASD who received naturalistic developmental behavioral interventions (NDBIs) as state-of-the-art treatment made achievements in cognitive skills, adaptive behaviors, and social communication skills.
Effective early interventions are an important priority for serving children and families; since families are now considered experts on their children, they often participate in implementing roles [8,9]. As children are at an early developmental stage, parent-implemented intervention (PII), an evidence-based practice, is highly recommended in the literature [10]. Recent research has shown that parents raising toddlers with ASD can acquire basic knowledge and implement teaching strategies, acting as interventionists in their toddlers’ daily lives [11,12]. Parents who learned about early development and ASD features were able to plan individualized interventions and successfully implement interventions throughout their daily routines [13,14]. Moreover, the parent-led group showed a significant increase in the length of jointly engaged time compared to the therapist-led group, and this increase was maintained at the 6-month follow-up [5].
Many efforts are being made to advance the timing of early interventions and to provide parents with effective interventions. For example, a university hospital in Hong Kong conducted parent training for 2 weeks while waiting for official services immediately after diagnosis and reported improvements in all areas and reduction of parental stress among toddlers who participated in education programs focused on social communication skills, such as eye contact, gesture, and language [15]. In Quebec, Canada, 94 toddlers with ASD and their parents were examined for 1 year to promote toddler development, and the study reported high parental satisfaction [16]. Stanford University Hospital in the United States provides free parental support programs to help parents raise autistic infants, providing effective links to early intervention services and achieving high parental satisfaction [17]. Florida State University Hospital further supports community early intervention programs [18].
The rapid increase in the incidence of ASD has significantly affected Korean medical and educational sites that support toddlers. Many families of children with early ASD symptoms seek services before a formal diagnosis due to delays in expressive language development and social interaction skills. Despite the recognized importance of early interventions, in Korea, group studies verifying the effectiveness of interventions for toddlers with ASD and their parents are limited [19]. Moreover, Studies that targeted both toddlers with ASD and their parents conducted on related topics over the past 5 years have varied in terms of the age, period, intervention method, and intensity of the programs of the participating toddlers and their parents. Additionally, early interventions or parental support programs provided by the public system for toddlers and parents affected or at risk of ASD are implemented to a very limited extent. Therefore, it is necessary to evaluate the performance of interventions through practical application. Furthermore, after the outbreak of coronavirus disease 2019 (COVID-19), toddlers with ASD and their parents experienced restrictions on the use of special education services, and most face-to-face parental education programs were canceled or conducted intermittently. These issues have prompted a need for alternative methods to increase the individual accessibility of services for parents of children with ASD by merging non-face-to-face methods with existing education programs and reducing the cost and time of direct visits. This study aimed to develop and investigate the effectiveness of a hospital-provided hybrid training program for parents of toddlers with or at risk of ASD.
Materials and Methods
1. Study population
The participants included 24 pairs of toddlers and parents residing in Seoul, Incheon, and Gyeonggi Province, in which the children were diagnosed with or the risk of ASD at the National Health Insurance Service Ilsan Hospital Development Delay Clinic. The inclusion criteria included: (1) toddlers younger than 34 months with ASD diagnosed by a child and adolescent psychiatrist; (2) as a result of a language evaluation, toddlers with speechlessness or delay (less than the 10th percentile compared with their peers); and (3) toddlers with Korean-Childhood Autism Rating Scale (K-CARS-2) scores of 30 or higher. Those who satisfied at least two of the above three criteria were included in this study. Fifteen pairs in the experimental group (12 boys and three girls; mean age, 29.7 months) and nine pairs in the control group (six boys and three girls; mean age, 30.1 months) participated in the study (Supplementary Table 1). The Levene test for equality of variance showed that the assumption of homogeneity of variance had not been violated for measures of age (t=-0.289, P>0.05) and K-CARS-2 scores (t=-0.716, P>0.05). There were two babies born prematurely (34+6, 36+1 weeks) in the experimental group and three (31, 34, 35 weeks) in the control group. There were no subjects with neurological diseases, including epilepsy, in either groups. The treatment intervention was defined as “a treatment to alleviate ASD, such as play therapy, language therapy, and sensory integration therapy, at least once a week for at least 3 months.” In the experimental group, no participants received other interventions. In the control group, only one participant received speech therapy and sensory integration therapy. There were no statistically significant differences between the two groups in terms of prematurity, history of neurological disease, and history of interventions for ASD. The researchers explained to the parents the purpose of the study and gave them brief guidance on the program. Parents who agreed with the procedures of the study signed an informed consent form and received an explanation that their personal information would remain confidential. The control group received no parent education program. The study period was from September 2020 to August 2021. This research was approved by the Medical Sciences Ethics Committee of Ilsan Medical Center (IRB file No. 2020-04-018).
2. Methods
1) A hospital-provided hybrid parental support program
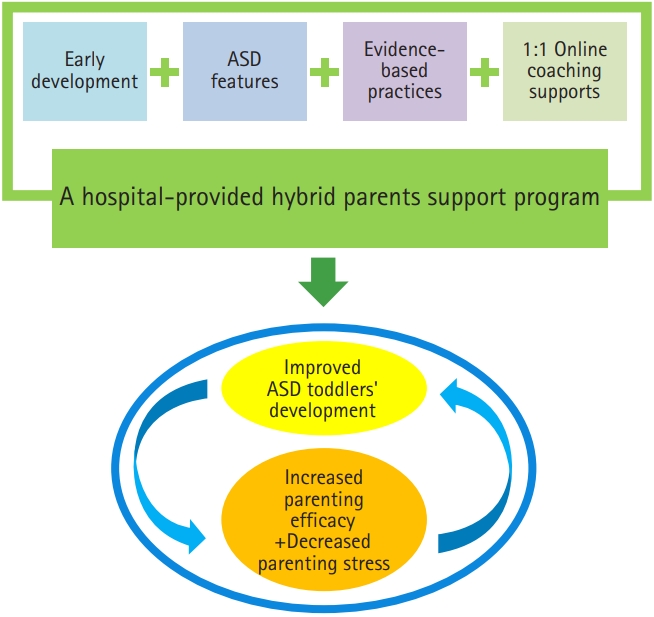
The hospital-provided hybrid parental support program was designed to reinforce parents’ capabilities and promote the development of toddlers with or at risk of ASD by delivering information to their parents and supporting the implementation of interventions. To construct the content and methods of this program, published NDBI manuals for young children with ASD, such as the Social Communication Emotional Regulation Transactional Support, were reviewed, focusing on the needs for parental support, the implementation method that parents want, and the teaching strategies of the existing parent support programs [10,11,20]. The specific implementation stages and content of the parental support program were organized as shown in Fig. 1.
The researchers of this study led the first to third and eighth group sessions in hospitals, and the risk of mass infection was minimized by separating the seats by 2 m and requiring all participants to wear a mask. The fourth to seventh sessions were conducted online using Zoom, an online-based platform, by a member of the research team with a PhD in the field of special education and autism. In the first and second sessions, rapport with participants was formed, and education on the characteristics of toddlers with ASD and early developmental features was covered. Parents watched extensive video footage from a web-based instructional program developed by the Florida State University Autism Institute. Observations, discussions, and questions and answers were conducted in the order of homework guidance. During the third session, the researchers helped parents set intervention goals based on the child’s behavioral observation data collected by parents in their daily lives. From the fourth to seventh sessions, the member of the research term with a PhD in special education conducted individual online sessions for about 90 minutes per week. Each week, the recent status was shared with parents who observed their children’s behavior, and a teaching plan that could be implemented in daily life was established following the progress of each session. In the fourth session, an interaction strategy that included following the child’s interest and imitating the child’s actions and verbalizations was covered. In the fifth session, behavioral teaching strategies, such as using natural reinforcement, time-delay, and the mand-model, were introduced. In the sixth session, information on children’s different sensory preferences, the types of play that reflects sensory profiles, and modeling were covered. In the seventh session, the use of visual support strategies and picture exchange communication systems was introduced, and all teaching strategies were reflected in the intervention plan. The researchers guided them to carry out interventions at home from the end of the session until the day the next session began. In the last session, group education was conducted at the hospital, reviewing the teaching strategies and providing guidance for future directions of interventions. The roles of the researchers and parents in each session are shown in Table 1.
2) Measures
In this study, the Early Social Communication Scales (ESCS) [21], K-CARS-2 [22], Korean Vineland Adaptive Behavior Scales-II (K-Vineland-II) [23], and the Korean version of Child Behavior Checklist for Ages 1.5-5 (K-CBCL 1.5-5) [24] were used to examine the key autism-related characteristics of toddlers with or at risk of ASD. The ESCS is a semi-structured observation measurement tool developed by Mundy and Gomes [21] to evaluate the nonverbal communication capabilities of infants and toddlers aged 8 to 30 months. The ESCS has been used to evaluate the social communication skills of infants and toddlers with ASD in previous studies. The interrater reliability was reported in previous studies [25] to be 91, and the variables measured in this study were the total frequency of responding to joint attention (RJA) and initiating joint attention (IJA). To evaluate changes in parental behavior, the measurements and results were analyzed using the Toddler Care Questionnaire (TCQ) [26] and the Korean Parenting Stress Index Short Form (K-PSI-SF) [27]. This was conducted twice, once before and once after the parental support program (Supplementary Table 2) [22, 23, 28-31].
3) Experimental design and procedures
A pretest-posttest control group design was used to ascertain whether behavioral changes between the two groups differed significantly. The control group received no education program or support over the same period of time.
4) Observer training and interobserver reliability
Before evaluating changes in the joint attention behavior of toddlers in the experimental group, the reliability between observers was secured by conducting observer training. After familiarization with the items of the ESCS and the operational definition for each question, two observers observed video clips of toddlers in the risk group who did not participate in this study, and further evaluated their behavior. The reliability between observers was calculated as an equivalent correlation coefficient (r). It has been recommended to conduct observer training until an r of 0.85 or higher is reached [32], while referring to the criteria of previous studies [25]. The training was terminated when r was 0.91. The evaluation was conducted by two observers, one from the research team and one who was not involved in other aspects of the study and was blind to both pretest and posttest conditions. The observers coded the video clips according to ESCS manual. The correlation coefficient between observers for the evaluation results was 0.90 for the pretest and 0.91 for the posttest.
5) Social validity for the study
To examine the social validity of the study, parents were asked to rate and score 15 questions on the appropriateness of the content, teaching strategies, education programs, appropriateness of procedures and methods, and competency reinforcing and generalization through the intervention, on a 5-point scale.
6) Intervention fidelity of the study
Intervention fidelity was evaluated by the researcher, Minkyung Suh by checking the record sheet to ascertain whether the researcher operated according to the plan for group education and one-on-one online sessions. The evaluation sheet comprised a total of 23 questions. Implemented or non-implemented items were recorded as “O” and “X” respectively. If not applicable, the items were recorded as “NA” (Table 2). Parent participants were evaluated by checking the treatment integrity record sheet to ascertain whether the intervention was carried out according to the plan from the fourth session conducted online. The fidelity of the parental intervention was calculated by recording 15 questions as “O” for items implemented by parents, and “X” for non-implemented questions (Table 3). The researcher, MinKyung Suh self checked the intervention fidelity form inspection data during the next visit
3. Statistical analysis
Data were analyzed using the Korean version of SPSS version 25.0 (IBM Corp., Armonk, NY, USA). The Mann-Whitney U test was used to compare differences between two groups, with significance accepted at a P value <0.05. The Wilcoxon rank test was used to compare the pretest and posttest differences between the experimental group and the control group.
Results
1. Changes in the behaviors of toddlers and parents in the experimental group
In the experimental group, the IJA scores on the ESCS increased from 1.40 (standard deviation [SD], 1.35) in the pretest to 3.53±1.36 in the posttest . The difference was statistically significant (P<0.01). The mean RJA score increased from 35.70±29.58 to 59.04±21.34. The difference was statistically significant (P<0.01). The K-CARS-2 scores of the experimental group decreased from 28.67±4.03 to 22.70±6.33; this difference was also statistically significant (P<0.01). The adaptive behavior composite score of the K-Vineland-II decreased from 71.47±10.10 to 69.47±11.65; the difference was not statistically significant. The total behavior composite score of the K-CBCL 1.5-5 decreased from 58.33±14.67 to 56.80±16.46; the difference was not statistically significant.
The parenting efficacy increased from 121.40±36.14 to 145.20±18.56; the difference was statistically significant (P<0.05). The parenting stress level of the experimental group increased from 95.07±19.54 to 98.33±21.50; this difference was likewise not statistically significant (Table 4).
2. Changes in the behavior of toddlers and parents in the control group
In the control group, from the pretest to the posttest, the K-CARS-2 scores decreased from 28.1±3.30 to 27.44±2.92; the difference was not statistically significant. The total behavior composite score of the K-CBCL 1.5-5 increased from 53.00±12.12 to 54.00±16.16; this difference was likewise not statistically significant.
The parenting efficacy increased from 133.56±11.57 to 136.11±17.24, and this difference was not statistically significant. The parenting stress level decreased from 95.44±17.19 to 89.22±17.24; this difference was also not statistically significant (Table 5).
3. Changes in the behavior of toddlers and parents between the experimental and control group
The difference in K-CARS-2 scores between the experimental and the control groups was statistically significant (Z=-2.63 and P<0.01). However, the difference in total behavior problem scores of the K-CBCL 1.5-5 between the two groups was not statistically significant.
The difference in parenting efficacy between the experimental and the control groups was statistically significant (Z=-2.12 and P<0.05). However, the difference in parenting stress between the two groups was not statistically significant (Table 6).
Discussion
The toddler participants in the experimental group showed significant improvements in their joint attention scores of the ESCS and K-CARS-2 scores from the pretest to the posttest. Additionally, parent participants showed a between-group difference in parenting efficacy that was statistically significant. The satisfaction with the program was high, confirming that it had a positive effect on the parents’ implementation of interventions. The main results of this study are discussed below.
First, this hospital-provided hybrid parental support program increased the joint attention skills of toddlers in the experimental group, and the difference between the pretest and posttest was statistically significant (P<0.01). This promising finding is consistent with a previous study by Kasari et al. [5], who reported the improvement of joint attention skills in toddlers via PIIs. Parents who participated in the study developed an overall understanding of ASD at 1 to 3 weeks by observing their children and learning specific strategies through an online session that lasted for 4 weeks. The fact that parents followed their children’s interests induced joint attention using preferred toys and provided repeated opportunities in their daily lives, which is believed to have influenced the increase in joint attention skills.
Second, the adaptive behavior, emotions, and behaviors of toddlers in the experimental group decreased. However, the difference between the pretest and the posttest was statistically insignificant. This result differs from the effect of online training on parents of toddlers with ASD for 12 weeks reported by Vismara et al. [33]. It appears that the 8-week period in this study was insufficient to achieve statistically significant results [33].
Third, the parenting efficacy of parents who participated in this study increased, and the between-group difference was statistically significant. This supports related studies [11,34], according to which a program conducted on toddlers with ASD and their parents affected parental parenting efficacy. In many cases, parents of ASD children said that poor information after diagnosis and the widely varying opinions of many experts delayed educational decisions and negatively affected parenting efficacy [35].
Fourth, the parenting stress level decreased over time for parents in the control group, whereas it increased in the experimental group. This finding is consistent with the results of a previous study that compared two parent education programs [5]. Parents came to better understand their children’s behavior during the online sessions, but the fact that they had to do homework and conduct interventions might have been a burden. It is believed that the parents’ feelings of worrying about their children’s behavior while conducting the intervention affected parenting stress. There are mixed research results on parenting stress depending on the child’s age, parents’ experiences, parents’ disability acceptance level, and the dose of the intervention [5,14]. Among these, the frequency and length (dose) of the intervention may be important factors in improving outcomes for parent stress [36]. It is therefore assumed that an extended parent education program would significantly contribute to relieving parenting stress.
The clinical implications of these findings are as follows. First, parents of young children with ASD are able to implement interventions daily. Second, a hybrid parent education format is an alternative to efficiently operate the program under circumstances where it is challenging to visit hospitals or have professionals visit homes owing to COVID-19. Third, professional support seems to have reinforced the parents' ability to implement interventions. From the first session, parents observed their child’s behaviors, types of play, preferred play objects, and were able to gradually increase the amount of cooperative play time by merging various teaching strategies.
The limitations of this study are as follows. First, toddlers older than 34 months at the start of the study could not participate in this study. Due to the small number of participants, this study could not be conducted as a randomized controlled trial, which remains a limitation of the study. Second, a limited number of parents were recruited, which is a drawback. In subsequent studies, it will be necessary to examine the effects on joint attention, adaptive behavior, emotion, and behaviors comprehensively, using a larger group of participants from various regions. Third, the parents had to visit hospitals to participate in the children’s tests and group education. Conducting the sessions at a preferred time could result in high participation.