Acute disseminated encephalomyelitis (ADEM) is an inflammatory demyelinating disorder of the central nervous system (CNS), with a relatively high incidence in the pediatric population [1]. Although the precise pathogenesis is unknown, ADEM is presumed to be an autoimmune disorder stimulated by a systemic infection or vaccination [2]. Aberrant immune reactions in ADEM are associated with several pathogens, including viruses (such as varicella, influenza virus, Epstein-Barr virus, enterovirus, and severe acute respiratory syndrome coronavirus 2) and bacteria (such as Mycoplasma pneumoniae and Streptococcus) [2]. Intussusception is one of the most common causes of intestinal obstruction [3]. The pathogenesis of intussusception without anatomical leading points remains unknown. However, intestinal lymphoid hyperplasia stimulated by infectious pathogens may cause intussusception [3]. We present an unusual case of ADEM accompanied by intussusception secondary to M. pneumoniae infection.
A previously healthy 17-month-old Korean girl was referred to our department with poor feeding, vomiting, decreased activity, and cyclic irritability following a 4-day prodromal illness consisting of cough, sputum, and mild fever. On admission, her body temperature was 37.7°C. Auscultation of both lung fields and the abdomen revealed bilateral crackles and decreased bowel sounds, respectively. Chest radiography revealed showed bilateral perihilar interstitial infiltrates (Fig. 1A). Her initial blood test result revealed no abnormalities, except for leukocytosis (12.3×109/L white blood cells) and a mildly increased serum C-reactive protein level (0.7 mg/dL; reference range, <0.5 mg/dL). Multiplex real-time polymerase chain reaction (PCR) results for respiratory viral and bacterial pathogens in nasopharyngeal aspirate were negative, except for M. pneumoniae. The result of an M. pneumoniae-specific immunoglobulin M antibody test was positive (3.30 immune status ratio [ISR]; reference range <0.8 ISR). Although the patient did not have stool mixed with blood and mucus, gastrointestinal ultrasonography was performed because of cyclic irritability. An ultrasound image showed the typical findings of intussusception (Fig. 1B and C) and the enlargement of several lymph nodes within the intussuscipiens, which may have been a leading point. The condition was diagnosed as ileocolic intussusception. She was treated with roxithromycin for M. pneumoniae and non-operative reduction using pneumatic pressure by enema for intussusception. Her respiratory symptoms improved; however, she presented with intermittent irritability and crying. Repeated gastrointestinal ultrasonography revealed successful reduction of intussusception with residual mesenteric lymphadenopathy.
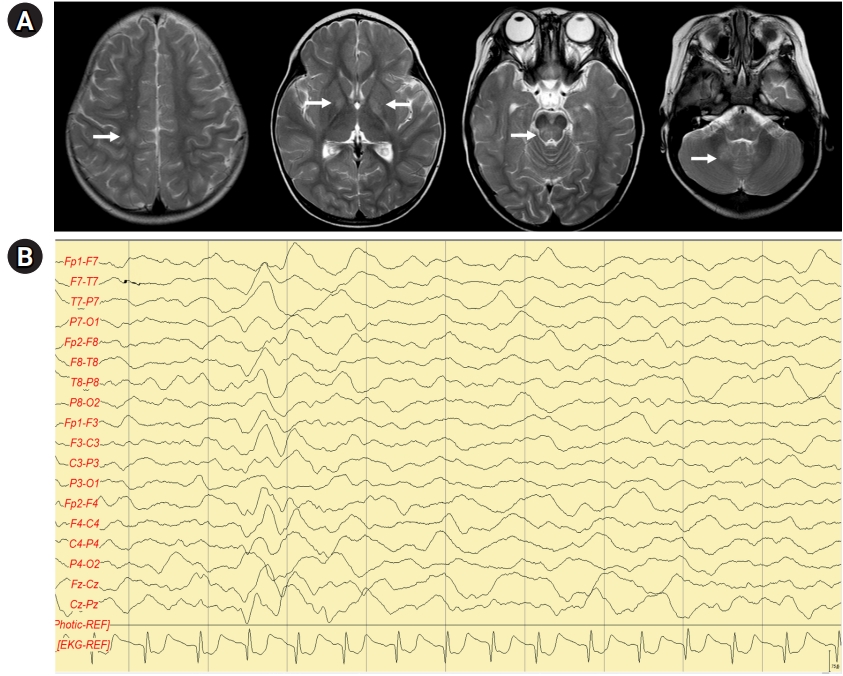
On day 5 of hospitalization, the patient abruptly showed drowsiness and a decreased response to stimulation. She could not sit unassisted, say meaningful words, or make eye contact. Brain magnetic resonance imaging (MRI) demonstrated multifocal T2 hyperintense lesions in the dentate nucleus, basal ganglia, posterior limb of the internal capsule, right centrum semiovale, and pons (Fig. 2A), suggesting ADEM. Sleep electroencephalography revealed generalized continuous slow waves without normal sleep patterns (Fig. 2B). Cerebrospinal fluid (CSF) analysis revealed no abnormalities, including cell counts and protein and glucose levels. Blood, urine, and CSF cultures showed no growth, and CSF PCR results for enterovirus, herpes simplex virus types 1 and 2, varicella-zoster virus, cytomegalovirus, measles, human herpesvirus 6, Mycobacterium tuberculosis, and M. pneumoniae were negative. The patient was seronegative for antibodies against myelin oligodendrocyte glycoprotein and aquaporin-4.
A diagnosis of ADEM secondary to M. pneumoniae infection was made. Intravenous methylprednisolone pulse therapy at 30 mg/kg/day was administered for 5 days, followed by oral prednisolone tapering for 3 weeks. On day 16, the patient’s mental status and eye contact improved. She could walk unassisted and speak meaningful words. On day 20, she was discharged with oral prednisolone on a tapering schedule. Three months later, she had completely recovered with no brain lesions on follow-up MRI. The patient maintained normal development, without recurrence of clinical symptoms at a 1-year follow-up.
The requirement for written informed consent was waived due to the retrospective nature of the study. The research was approved by the Institutional Review Board of Inje University Busan Paik Hospital (Busan, Korea; approval number: 2022-09-010).
ADEM is a heterogeneous demyelinating disorder of the CNS that has historically been inconsistently defined [1]. The International Pediatric Multiple Sclerosis Study Group has proposed and updated the following criteria for ADEM in 2013 [4]: (1) a first polyfocal, clinical CNS event with a presumed inflammatory demyelinating cause; (2) encephalopathy not explained by fever, systemic illness, or postictal symptoms; (3) no new clinical and MRI findings emerging 3 months or more after the onset; (4) abnormal brain MRI during the acute phase, with a diffuse, poorly demarcated, large lesion greater than 1 to 2 cm, predominantly involving the cerebral white matter, or a deep gray matter lesion in the thalamus or basal ganglia [4]. All the above-mentioned diagnostic criteria for ADEM were met in our patient.
The pathogenesis of ADEM caused by M. pneumoniae is not clear. M. pneumoniae has been postulated to directly invade the CNS or indirectly stimulate immune-mediated reactions, such as the production of autoantibodies with cross-reactivity to myelin [5]. Considering the long latent period between infection and ADEM and a good response to anti-inflammatory or immune-modulating drugs, an immune-mediated pathomechanism seems more reasonable [5]. Initially, our patient presented with prodromal symptoms, including a mild fever and respiratory symptoms. Respiratory symptoms improved after treatment with roxithromycin. Neurological signs, such as drowsiness and altered mental status, began approximately 9 days after the prodromal symptoms. It is unclear whether repetitive irritability was a symptom of ADEM, as the patient may have had intussusception- or mesenteric lymphadenopathy-associated irritability. Several cases of mycoplasma infection-associated ADEM have been reported to involve immune-mediated demyelination following respiratory infection; in those cases, the bacterium was detected in respiratory samples but not in CSF samples, as in our case [5-8]. Furthermore, our patient showed an excellent response to steroid pulse therapy, indicating an immune-mediated etiology of ADEM secondary to mycoplasma infection.
At the first visit to the hospital, our patient presented with ileocolic intussusception, presumably caused by mycoplasma infection. Abdominal ultrasonography revealed mesenteric lymph node enlargement. Lymphadenopathy associated with viral or bacterial infections can trigger intussusception [3,9]. Since gastrointestinal manifestations are the most common extrapulmonary symptoms in M. pneumoniae infection [10], our patient might have had intussusception due to the bacterium-associated enlargement of numerous mesenteric lymph nodes.
This report describes the first case of ADEM accompanied by intussusception following M. pneumoniae infection. Pediatricians should be familiar with the extrapulmonary symptoms of M. pneumoniae infection. Although rare, ADEM secondary to mycoplasma infection should be considered in patients with neurological symptoms. The treatment includes intravenous steroids or other immune-modulating drugs and antimicrobial therapy to treat the underlying infection. A gastrointestinal examination is also necessary in patients with abdominal symptoms, such as vomiting, pain, and cyclic irritability, during the acute phase of mycoplasma infection.