Assessment of Parenting Attitudes by Children and Adolescents with Migraine
Article information

Abstract
Purpose
We aimed to investigate the parenting attitudes reported by patients and their relationships with the characteristics of headaches in children and adolescents with migraine.
Methods
We conducted a retrospective review of medical records of children and adolescents with migrainous headaches (n=115; 59.1% female; mean age, 11.89±2.00 years). Children evaluated parental attitudes using the Parenting Attitude Test-Youth (PAT-Y), which comprises eight subscales and four newly devised secondary subscales. Headache severity was calculated by the visual analog scale (VAS), monthly frequency (MF), and VAS×MF/4 (VF). The scores of PAT-Y subscales and the correlations between PAT-Y scores and headache severity were analyzed by age group and sex. Scores for children’s depression inventory, childhood behavior checklists, and an attention deficit hyperactivity disorder scale were also analyzed.
Results
In the elementary school age group, VAS was weakly negatively correlated with the “achievement press” (r=–0.28, P<0.05) and “high expectation” (r=–0.25, P<0.05) attitudes, and VF was weakly negatively correlated with “achievement press” (r=–0.32, P<0.05), “punishment” (r=–0.27, P<0.05), and “high expectation” (r=–0.29, P<0.05). In the middle-school age group, MF and VF were moderately positively correlated with the “achievement press” attitude (r=0.48, P<0.01 and r=0.48, P<0.01, respectively), VF was weakly positively correlated with the “neglectful” attitude(r=0.31, P<0.05), and MF was weakly positively correlated with scores for depression (r=0.29, P<0.05) and internalized problems (r=0.31, P<0.05).
Conclusion
Parenting attitudes perceived by children and adolescents with migrainous headaches varied by age, and some parenting attitudes were related to headache severity. Education on age-appropriate parenting attitudes may help cope with migrainous headaches.
Introduction
Headache is one of the most common neurological symptoms in children. Among the various causes of recurrent acute headaches, migrainous headaches are a common condition without organic causes. The prevalence of pediatric migraine was reported to be 7.7% to 9.1% [1,2], with 4% to 11% in children 7 to 11 years of age and up to 8% to 23% in adolescents [1-4]. The prevalence is similar in both sexes, but pediatric migraine is more common in girls before adolescence [2]. Although migraine is usually a benign condition, uncontrolled headaches can cause various impairments in activities of daily living.
Parenting attitudes refer to the behavioral patterns and attitudes of primary caregivers that manifest when raising children. Parenting attitudes tend to be consistent during parenting [5], although they may influence or be influenced by disease-related attitudes or behaviors of children with migraine. Researchers have classified parenting attitudes in several ways, mainly using dimensional approaches [6-9]. The most commonly referenced parenting attitude types, as suggested by Baumrind [10] (1971) are authoritative, authoritarian, permissive, and neglectful attitudes, based on the warmth and control dimensions [11]. One of the well-known methods of assessing parenting attitudes is the Parental Attitudes Determining Scale developed by Lamborn et al. [12] (1991), which consists of 26 items. In Korea, both the Parenting Attitude Test (PAT) (assessed by the parent) and the Parenting Attitude Test-Youth (PAT-Y) (assessed by youth) are tools that consider the cultural background of Kore [13].
There are few studies on parenting attitudes toward children with migrainous headaches. Studies have shown that parents of chronic migraine patients have higher oppressive-authoritarian attitudes than those of patients with other types of headache [14], and are more sensitive and overprotective regarding their children's health problems [15]. Higher age of patients was associated with negative parenting styles [14,16,17]. Previous studies on the relationship between headache characteristics and parenting attitudes have shown that the ambivalent attachment style was associated with high attack frequency and pain intensity in children with migraine [18]. However, other studies found no significant relationships between headache severity and parenting attitudes [14]. Nonetheless, detailed reports on the parenting attitudes of children with migraine or on differences according to children’s age group remain scarce. Evaluating parenting attitudes from the perspective of children can provide valuable information for understanding headache-related behaviors or for the provision of family counseling.
In the present study, we investigated parenting attitudes as perceived by children with migraine and investigated the relationship between headache severity and parenting attitudes. We hypothesized that the parental attitudes perceived by youth may be different in children and teenagers. The analyses were first performed among children of all ages and then separately for elementary-school age group (ESAG) and middle-school age group (MSAG).
Materials and Methods
1. Patients
We retrospectively reviewed the data of patients treated between March 2014 and November 2019 at the Pediatric Department of Hanyang University Guri Hospital. The inclusion criteria were patients 8 to 15 years of age who were diagnosed with migraine or probable migraine and underwent testing with a battery of behavioral checklists, including the PAT-Y. We excluded patients with migraine-related episodic syndrome.
2. Clinical data
Migraine was diagnosed based on each patient’s history, physical examination, and neurological examination. For clinical data, age, sex, and characteristics of headache were analyzed. In the present study, we included patients diagnosed with migraine with aura, migraine without aura, and probable migraine. The diagnosis of migraine was re-evaluated during data analysis based on the International Classification of Headache Disorders, third edition [19]. Headache severity was calculated by visual analog scale (VAS) (range, 1–10; no pain, 0; worst pain, 10), monthly frequency (MF) (number of times of headache occurrence per month), and VAS×MF/4 (VF) score. This study protocol was approved by the Institutional Review Board of Hanyang University Guri Hospital (IRB reference no: GURI 2022-01-018). Written informed consent by the patients was waived due to a retrospective nature of our study.
3. Behavioral scales
1) Parenting Attitude Test-Youth
The PAT-Y was developed by Lim and Lee [13] to evaluate parents' parenting attitudes, which are estimated by children using items that are highly related to emotional exchange and behavioral expression between parents and children. It consists of 43 items, each of which is answered on a 5-point Likert scale, and has the following eight subscales for parenting attitudes [13]: “supportive expression,” “rational explanation,” “achievement press,” “high involvement,” “punishment,” “superintendence,” “high expectation,” and “inconsequence.” The PAT-Y provides a raw score, percentile scores, and appropriate percentile ranges for each scale. After obtaining scores for the eight primary subscales, we recalculated them into four secondary subscales, corresponding to authoritative, authoritarian, permissive, and neglectful attitudes. Therefore, 12 subscales were used for the analysis in the present study.
2) Korean Children’s Depression Inventory
The Korean Children’s Depression Inventory (K-CDI) is a self-reported scale used to evaluate the emotional, cognitive, and behavioral symptoms of depression in children and adolescents. It consists of a total of 27 items, and a score of ≥22 is considered to indicate depression. In the present study, the total score was used for analysis [20].
3) Korean Child Behavior Checklists 6-18
The Korean Child Behavior Checklists 6-18 (K-CBCL 6-18) are used for early identification and diagnosis by evaluating emotional and behavioral problems in children and adolescents using reports from primary caregivers. There are eight subscales within the problem behavior scale: anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, delinquent behavior, and aggressive behavior. These subscales can be grouped into two higher-order factors, known as internalizing and externalizing problems. In the present study, percentile scores of internalizing and externalizing problems scales were used for analysis [21,22].
4) Korean Attention Deficit Hyperactivity Disorder Rating Scale-IV
The Korean Attention Deficit Hyperactivity Disorder Rating Scale-IV (K-ARS-IV) [23,24] consists of 18 items with 4-point scales (0–3). The total score of odd-numbered items measures attention deficit symptoms, and the total score of even-numbered items measures hyperactivity-impulsivity symptoms. If the total score is ≥19 based on the parental evaluation and ≥17 according to the teacher’s evaluation, a child is considered to have attention deficit hyperactivity disorder (ADHD) [25]. In the present study, parental evaluation was conducted, and the total score was used for the analysis.
4. Statistical analysis
The demographic characteristics of the study population are presented as mean±standard deviation and range for continuous variables and as frequency (percentage) for categorical variables. The independent two-sample t-test was performed to compare differences in demographic and behavioral scales in total and by age group. Pearson correlation analysis was performed to analyze the relationships between behavioral scales and headache severity (VAS, MF, and VF). The statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). A P<0.05 was considered statistically significant.
Results
1. Clinical characteristics
In total, 115 patients were finally included in the analysis (female, 59.1%; mean age, 11.89±2.00 years). The 62 children attending elementary school (mean age, 10.32±1.30 years; range, 8 to 12) and 53 adolescents attending middle school (mean age, 13.71±0.66 years; range, 13 to 15) were grouped as the ESAG and the MSAG, respectively.
The mean MF of headaches was 12.93±10.03 times/month (range, 0.2 to 28), and the mean VAS was 5.78±1.92 (range, 2 to 10). The mean VF score was 18.33±16.47 (range, 0.2 to 70). Details of the characteristics are presented in Table 1.
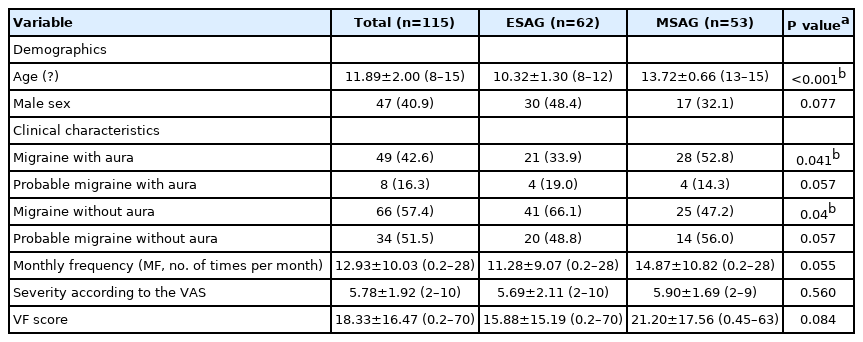
Baseline demographic and clinical characteristics of patients
2. Behavioral scales
1) PAT-Y
The mean percentile scores for the eight primary parenting attitude subscales ranged from 46 to 60 (ESAG, 50 to 58; MSAG, 43 to 63). The mean percentile scores for four secondary subscales ranged from 49 to 55 (ESAG, 45 to 54; MSAG, 43 to 58). The mean distributions were generally in or around the middle range. The mean scores were more widely distributed in the MSAG than in the ESAG (Supplementary Table 1).
In all age groups, the mean percentile of ”supportive expression” was significantly higher in males than in females (57.13±28.82 vs. 43.22±28.08, P=0.011); in particular, the ESAG (63.33±22.91 vs. 44.56±30.70, P=0.009) showed significantly higher scores in males. In the MSAG, “achievement press” was significantly higher in males than in females (59.71±18.07 vs. 41.75±26.36, P=0.014). Supplementary Table 1 presents the results in detail according to age group.
Overall, the scores for positive parenting items as perceived by the patients tended to be higher in the ESAG than in the MSAG, and the scores for negative parenting items tended to be higher in the MSAG than in the ESAG. In particular, the mean percentile scores for “rational explanation” (54.58±30.56 vs. 43.30±29.65, P=0.048) and ”authoritative parenting” (54.11±27.48 vs. 43.33±27.91, P=0.04) attitudes were higher in the ESAG than in the MSAG, and that for “high expectation” (46.24±30.26 vs. 61.06±26.71, P=0.007) was significantly higher in the MSAG than in the ESAG. The differences in parenting indices according to age group are shown in Fig. 1. The PAT-Y subscales were also compared based on the classification of patients with migraine according to whether they did or did not experience auras, and this analysis showed no significant difference (Supplementary Fig. 1).
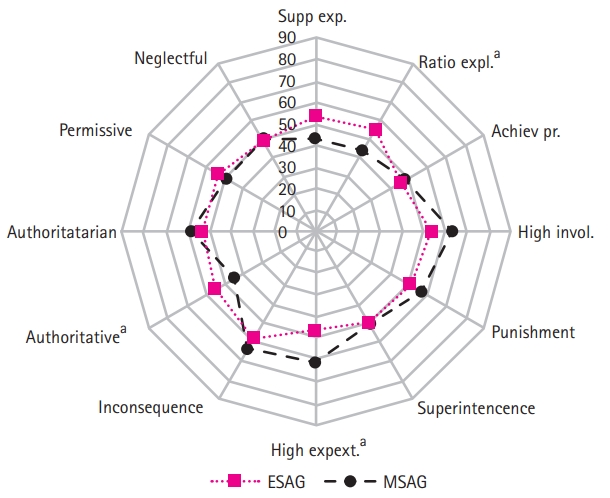
Comparison of Parenting Attitude Test-Youth (PAT-Y) subscales between the elementary-school age group and middle-school age group. The radial axis indicates the percentile scores of PAT-Y subscales. Supp exp., supportive expression; Ratio expl., rational explanation; Achiev pr., achievement press; High invol., high involvement; High expect., high expectation; ESAG, elementary-school age group; MSAG, middle-school age group. aP<0.05.
2) K-CDI, K-CBCL 6-18, and K-ARS-IV
In all age groups, the mean score of CDI was 11.34±7.51, which was significantly higher in females than in males (12.60±8.06 vs. 9.51±6.27, P=0.029). The mean CDI score was significantly higher in the MSAG than in the ESAG (13.28±7.06 vs. 9.68±7.54, P=0.01) (Supplementary Table 2).
The mean percentile score for internalizing problems in the K-CBCL showed no significant difference based on age group or sex. However, the mean percentile score for externalizing problems in the MSAG was significantly higher than that of the ESAG (66.92±25.31 vs. 56.42±26.00, P=0.032) (Supplementary Table 2).
In all age groups, the mean score for inattention (4.85±5.00 vs. 3.24±3.48, P=0.045), hyperactivity-impulsivity (2.89±3.48 vs. 1.40±2.18, P=0.006), and ADHD-total (7.74±8.09 vs. 4.64±5.24, P=0.014) were significantly higher in males than that in females. The mean score of ADHD scales was not significantly different according to sex in the ESAG. However, in the MSAG, the mean scores for inattention (6.71±5.90 vs. 3.78±3.58, P=0.029), hyperactivity-impulsivity (3.76±4.12 vs. 1.42±2.10, P=0.008), and ADHD-total (10.47±9.70 vs. 5.19±5.26, P=0.013) were significantly higher in males than in females (Supplementary Table 2).
3) Correlation between PAT-Y and headache severity
In all age groups, there was no clear correlation between the frequency and intensity of headache and parenting attitudes, with only very weak, significantly negative correlations between MF and the “authoritative parenting” attitude (r=–0.19, P<0.05) and between VF and the “rational explanation” attitude (r=–0.19, P<0.01) (Table 2).
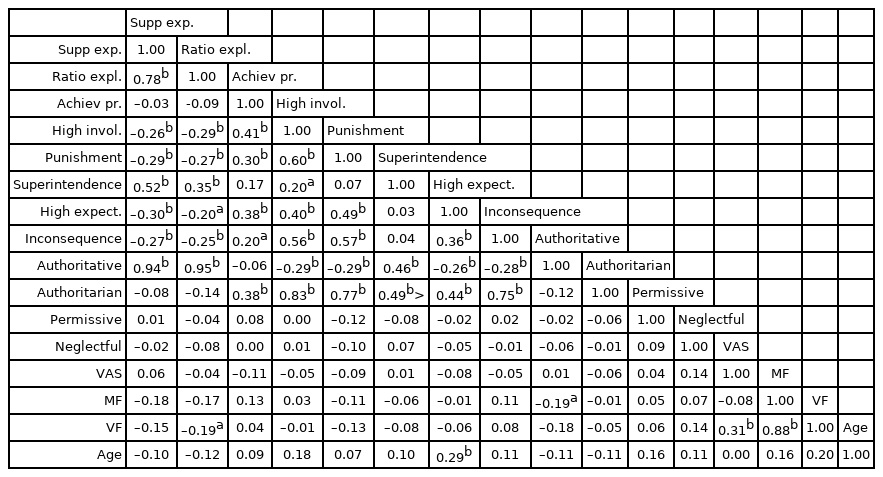
Correlation matrix between Parenting Attitude Test-Youth and headache severity in all age groups
In the ESAG, VAS showed weak negative correlations with “achievement press” (r=–0.28, P<0.05) and “high expectation” (r=–0.25, P<0.05), and VF showed weak negative correlations with “achievement press” (r=–0.32, P<0.05), “punishment” (r=–0.26, P<0.05), and “high expectation” (r=–0.29, P<0.05) (Table 3).

Correlation matrix between Parenting Attitude Test-Youth and headache severity in the elementary-school age group
In the MSAG, age showed a weak positive correlation with “superintendence” (r=0.34, P<0.05), and MF and VF showed moderate positive correlations with “achievement press” (r=0.48, P<0.01 and r=0.48, P<0.01, respectively). VF also showed a weak positive correlation with the “neglectful” attitude (r=0.31, P<0.05) (Table 4).

Correlation matrix between Parenting Attitude Test-Youth and headache severity in the middle-school age group
4) Correlation between other behavioral scales and headache severity
In all age groups, there was no clear correlation between the frequency and intensity of headache and other behavioral scales, with only very weak, significantly positive correlations between MF and VF and the internalizing problem score of the K-CBCL (r=0.20, P< 0.05 and r=0.21, P<0.05, respectively) (Supplementary Table 3).
In the analysis of MSAG, MF showed weak positive correlations with the CDI score (r=0.29, P<0.05) and internalizing problems (r=0.31, P<0.05), and VF showed a weak positive correlation with the internalizing problems (r=0.34, P<0.05) (Supplementary Table 4). However, in the ESAG, the frequency and intensity of headaches did not show significant correlations with other behavioral scales (Supplementary Table 5).
Discussion
In the present study, parenting attitudes perceived by youth differed between the ESAG and MSAG. Some parenting attitudes presented different relationships with the degree of headache by age group. In the ESAG, the headache intensity presented by VAS was negatively correlated with “achievement press” and “high expectation,” and the general severity score presented by VF was negatively correlated with “achievement press,” “punishment,” and “high expectation.” In the MSAG, the headache frequency measured by MF and the general severity score showed moderately positive correlations with “achievement press,” and VF showed a weakly positive correlation with the “neglectful” attitude.
Parenting attitudes refer to all attitudes and behaviors consistently displayed by primary caregivers regarding the desired growth and development of a child when raising a child. A desirable parenting attitude is to help children take responsibility for their own lives and have the ability to control their own behavior. It also helps to form good interpersonal relationships as they grow up and to develop self-esteem [13].
Although the importance of parental roles and parenting attitudes in managing headaches in children and adolescents has been emphasized, there are not many studies on parenting attitudes based on the patient’s perspective [14-17]. In previous studies on migraine patients, migraine was positively associated with anxiety symptoms, and parents of children with chronic migraine showed higher oppressive-authoritarian attitudes than those of other headache patients [14]. In addition, another study showed that parents of children with headaches were more sensitive to health problems and showed an overprotective attitude [15]. Higher age was associated with a negative parenting style [14,16,17].
To evaluate parenting attitudes, this study used the PAT-Y developed by Lim et al. [13]. It consists of eight primary subscales and four newly developed secondary subscales. The eight primary subscales include the verified attitudes of parenting. “Supportive expression” evaluates the degree of expression of affection by parents (the ideal range is around the 75th±10th percentile). “Rational explanation” quantifies the degree of effort that parents make to explain their children's mistakes so that they could understand them from the child's point of view when they rebuke them (the ideal range is the 75th±10th percentile). “Achievement press” assesses the degree to which parents strongly demand social success from their children (the ideal range is the 60th±10th percentile). “High involvement” evaluates the degree to which parents are reluctant to respect their children's privacy (the ideal range is the 50th±10th percentile). “Punishment” assesses the degree to which parents impose physical punishment or psychological threats on their children (the ideal range is the 40th±10th percentile). “Superintendence” quantifies the degree to which parents check their children's schedule (the ideal range is the 40th±10th percentile). “High expectation” evaluates the degree of parents’ implicit expectations (the ideal range is the 30th±10th percentile). “Inconsequence” assesses the degree of inconsistency in the standards of rebuke for their children's behavior (the ideal range is the 20th±10th percentile) [13].
In the present study, the range of mean percentiles of all patients for each of the eight subscales was generally in the middle of the scores (range, 46.22 to 60.46). However, there were differences according to the subscales. In general, the “supportive expression,” “rational explanation,” and “achievement press” scores were lower than the ideal ranges, and the “high expectation” and “inconsequence” scores were higher than the ideal ranges. The “high involvement,” “punishment,” and “superintendence” scores were in ranges similar to or slightly different from the ideal scores. The average scores of some attitudes did not meet the ideal ranges. Since it is often found that parental attitudes do not meet the ideal criteria in the general population [13], it is difficult to determine whether these results are characteristic of the families of headache patients.
‘Supportive expression’ perceived by patients was significantly lower in females than in males, especially in the ESAG. The reason why elementary-school girls perceived that they received less support from their parents is not clear. However, we suggest that parents of girls of this age group should express more support. The mean percentile score of “rational explanations” was significantly lower in the MSAG than in the ESAG. Parents need to increase their rational explanations in a way that adolescents can understand. The mean percentile score of “achievement press” was significantly higher in males than in females in the MSAG. This suggests that adolescent boys with headaches included in this study perceived more stress than girls by their parents because of schoolwork. However, the mean percentile scores of “achievement press” were lower than the recommended range of approximately the 60th percentile in these patients. As opposed to “rational expression,” the mean percentile scores of “high expectation” perceived by patients were significantly higher in the MSAG than in the ESAG. The mean percentile of “high expectation” for adolescents was twice as high as the recommended range. Adolescents’ perceptions that they are not meeting their parents' expectations can be a factor that lowers their self-esteem.
Four secondary subscales were newly developed by the authors for further analysis. The authoritative attitude was defined as the average of the “supportive expression” and “rational explanation” attitudes, which are usually positive attitudes. The percentile score of the authoritative attitude was significantly higher in the ESAG than in the MSAG. The authoritarian attitude was defined as the average of four subscales (“high involvement,” “punishment,” “superintendence,” and “inconsequence”). The permissive attitude was defined as 100–(the average of the percentile scores of “achievement press” and “high expectation”). The neglectful attitude was defined as 100–(the average of four subscales: “supportive expression,” “rational explanation,” “high involvement,” and “superintendence”). There were differences by age and sex in the authoritarian, permissive, and neglectful attitudes.
As in previous studies, no clear association between headache severity and parenting attitudes was found in all age groups, including both the ESAG and MSAG [14]. However, when analyzing correlations by age group, differences were found in the correlations for several parenting attitude items. In the ESAG, the intensity and frequency of headaches were lower when the scores for the “achievement press,” “high expectation,” and “punishment” attitudes were higher, but these correlations were slight. “Achievement press” and “high expectation” corresponded to non-permissive parenting attitudes, and the “punishment” attitude corresponded to authoritarian parenting. Although it is difficult to accurately interpret these correlations, it may be possible that the attitude of parents who do not accept pampering of their child may affect their child's expression of headaches. Whether authoritarian control is effective in reducing headache symptoms in the ESAG needs to be assessed in future studies. On the contrary, higher levels of non-permissive parenting, as exemplified by the “achievement press” and “neglectful” attitudes, were related to headache severity in the MSAG. This implies that during adolescence, parental pressure to study may increase pain, while indifference from parents may also increase the severity of headaches. Although these results should be interpreted carefully and also need further studies for validation, they imply that different parenting attitudes are related to the exacerbation of headaches in childhood and adolescence.
The use of self-reported questionnaires in evaluating parents' parenting attitudes may have limitations in accuracy. However, parenting attitudes as scored by children may be more closely related to the behavioral characteristics of children than to the parenting attitudes of the parents [26]. A strength of the present study is that this was the first study in Korea to assess and analyze parenting attitudes in migraine patients by age group. The limitations are that this is a retrospective study and could not be compared with controls or patients with other types of primary headaches.
Therefore, the importance of parenting attitudes in managing pain should be emphasized more strongly. Performing psychological and behavioral evaluations in the treatment of pediatric headaches would be helpful in establishing a comprehensive treatment plan for patients. The same parenting attitude may have different effects on children depending on their age. Adjusting the parenting attitude of parents according to the growth stage of their children will help to cope with headaches in these children.
Supplementary materials
Supplementary materials related to this article can be found online at https://doi.org/10.26815/acn.2022.00164.
Results of Parenting Attitude Test-Youth
Results of behavioral scales
Correlation matrix between other behavioral scales and headache severity in all age groups
Correlation matrix between other behavioral scales and headache severity in middle school age group
Correlation matrix between other behavioral scales and headache severity in elementary school age group
Comparison of Parenting Attitude Test-Youth (PAT-Y) subscales between migraine without aura and migraine with aura. The radial axis means percentile scores of PAT-Y subscales. Supp exp., supportive expression; Ratio expl., rational explanation; Achiev pr., achievement press; High invol., high involvement; High expect., high expectation; MO, migraine without aura; MW, migraine with aura.
Notes
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: JHM. Data curation: KML and MSK. Formal analysis: SR. Methodology: HL and JHM. Writing-original draft: KML. Writing-review & editing: YJK and JHM.
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF-2019R1F1A1058704).