Introduction
Neurofibromatosis type 1 (NF1) is one of the most common autosomal dominant disorders, with an estimated prevalence of about 1 in 3,000 individuals [1]. It is associated with a mutation in neurofibromin, a tumor suppressor protein located on chromosome 17q11.2.
The diagnostic criteria for NF1 were presented in a National Institutes of Health (NIH) statement in 1987. Two or more Lisch nodules in the iris were required as one of the criteria. Recent imaging technologies, such as near-infrared reflectance (NIR) imaging and optical coherence tomography (OCT), have enabled the visualization of choroidal abnormalities or nodules, which manifest as bright, patchy nodules in most NF1 patients. Therefore, the criteria for NF1 were revised in 2021, adding ŌĆ£two or more choroidal abnormalitiesŌĆØ as an ophthalmologic criterion [2]. Our group first reported choroidal nodules in a middle-aged Korean NF1 patient [3], but knowledge of choroidal nodules as an ocular manifestation in Korean NF1 patients has remained limited. Therefore, the present study investigated the clinical efficacy of NIR imaging and OCT to identify choroidal abnormalities in Korean children with NF1. Additionally, the frequency of choroidal abnormalities in Korean children with NF1 was investigated and compared with that of Lisch nodules.
Materials and Methods
This retrospective study was conducted at the Department of Ophthalmology at Inje University Sanggye Paik Hospital. It was approved by the Institutional Review Board of Inje University Sanggye Paik Hospital (approval number: 2022-04-001) and adhered to the Declaration of Helsinki. Written informed consent by the patients was waived due to a retrospective nature of our study.
This study included 10 eyes in five Korean children with NF1 (<18 years old) who had undergone NIR imaging or OCT scans (Heidelberg Engineering, Heidelberg, Germany) at the Department of Ophthalmology, Inje University Sanggye Paik Hospital, from January 2014 to April 2022. The diagnosis of NF1 was based on the stringent NIH criteria. All patients also underwent ophthalmic procedures, including slit-lamp examinations, NIR imaging, OCT scanning, and fundus examinations other than by NIR imaging or OCT.
Results
The data on the patients and their eyes are shown in Table 1. At the first visit, Lisch nodules were found in only two eyes. After our initial report on choroidal nodules found in a middle-aged Korean NF1 patient, NIR imaging and OCT scans were taken for pediatric NF1 patients in the course of their follow-up. Choroidal nodules were found in all eyes of all patients. Slit-lamp examinations performed on the same day as NIR imaging and OCT scans revealed two, one, two, and three Lisch nodules unilaterally in cases 1, 2, 3, and 5, respectively. To fulfill the criteria for NF1, two or more Lisch nodules are needed; however, in case 2, only one Lisch nodule was found, and in case 4, there was no Lisch nodule.
1. Case 1
A 4-month-old girl visited our clinic for congenital nasolacrimal duct obstruction. More than 15 caf├®-au-lait spots larger than 5 mm in the greatest dimension and freckling on the right axilla were discovered, though no slit-lamp examination could be performed due to poor cooperation. She visited our clinic regularly thereafter. When she was 2 years old, no Lisch nodule was found on her first slit-lamp examination, but one neurofibroma had newly appeared on her left hand. When she was 4 years old, her best-corrected visual acuity (BCVA) was 20/25 in the right eye and 20/50 in the left eye. One Lisch nodule was initially found in her right eye. Color fundus photography appeared normal in both eyes (Fig. 1A). One year later, two Lisch nodules were discovered in her right eye, whereas her left eye still showed no Lisch nodules. NIR imaging and OCT scanning were performed, revealing two choroidal nodules in the right eye, and three choroidal nodules, one of which was located within the macular area, in the left eye (Fig. 1A). OCT scans of the area of high reflectance in NIR imaging clearly showed the presence of a choroidal nodule with an irregular hyper-reflectance focus confined to the choroid (Fig. 1A). After another year, her BCVA was 20/25 in both eyes.
2. Case 2
A 5-month-old boy with more than 10 caf├®-au-lait spots larger than 5 mm was referred to our clinic for NF1 evaluation. There were no Lisch nodules on the initial visit. After that, he had regular check-ups every 6 months. When he was 1 year old, one neurofibroma was newly found at the nape of his neck. The BCVA, which was measured at 3 years old when he was able to cooperate, was 20/20 in both eyes. When he was 5 years old, one small hypo-pigmented nodule was found in the iris of his right eye. No Lisch nodules were found in the left eye. Color fundus photography showed no abnormalities (Fig. 1B). When the first NIR imaging and OCT were performed at the age of 8, four small choroidal nodules in the right eye and two choroidal nodules in the left eye were found (Fig. 1B). No additional Lisch nodules appeared in the course of his follow-up.
3. Case 3
A 4-year-old boy visited our clinic for esotropia. He had more than 10 caf├®-au-lait spots larger than 5 mm, freckles in the axilla, and had already been diagnosed with NF1 at another hospital. The BCVA was 20/25 in both eyes, and the alternative prism cover test showed 15-prism diopter left esotropia at distance and near. A slit-lamp examination revealed two Lisch nodules in the right eye, whereas no Lisch nodules were apparent in the left eye. No abnormalities were found on color fundus photography (Fig. 1C). NIR imaging and OCT after a month showed three choroidal nodules in the right eye and one small choroidal nodule in the left eye (Fig. 1C). After another 3 months, a Lisch nodule was newly found in the left eye.
4. Case 4
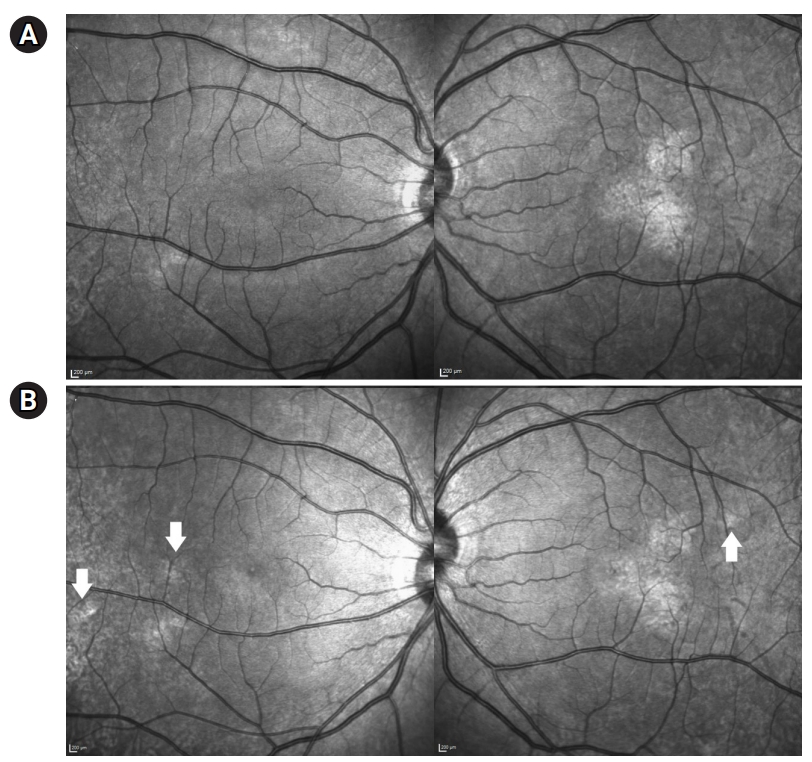
A 5-year-old boy was referred to our clinic for NF1 evaluation. He had 14 caf├®-au-lait spots larger than 5 mm, freckles in the axilla, and two neurofibromas in the anterior abdominal wall, and his mother had already been diagnosed with NF1. On the first visit, the BCVA in both eyes was 20/20. There were no visible Lisch nodules. He underwent the first NIR imaging and OCT scans 3 years after the first visit, which showed one choroidal nodule in the right eye and two choroidal nodules in the left eye. One of the choroidal nodules in the left eye was located within the macular region (Fig. 2A). Color fundus photography, taken on the same day, was normal (Fig. 1D). In the course of follow-up every 6 months, Lisch nodules still were unobserved. However, the choroidal nodules became more apparent. When he was 12 years old, the number of choroidal nodules had increased to 2 in the right eye and 3 in the left eye on NIR imaging (Fig. 2B).
5. Case 5
A 9-year-old boy, the sibling of case 4, was referred to our clinic for NF1 evaluation. He had 21 caf├®-au-lait macules larger than 5 mm, freckles in the axilla and groin, and one neurofibroma on the ankle. The BCVA of both eyes was 20/20. There were no Lisch nodules in the right eye, and two Lisch nodules were observed in the left eye. He revisited our clinic after 5 years. Lisch nodules remained absent from the right eye, while one additional Lisch nodule had appeared in the left eye, for a total of three. Color fundus photography was normal in both eyes (Fig. 1E). He underwent NIR imaging and OCT scanning on the same day, whereupon two choroidal nodules in the right eye and seven choroidal nodules in the left eye were found (Fig. 1E). Regular follow-up was done every 6 months, and by the time the patient was 15 years old, one Lisch nodule had appeared in the right eye.
Discussion
Our study, which is the first report on choroidal nodules in a case series involving Korean NF1 patients, showed that choroidal nodules outnumbered and developed earlier than Lisch nodules in Korean children with NF1,.
According to the previous diagnostic criteria developed at NIH in 1987, Lisch nodules, optic pathway glioma, and osseous lesions are the only extra-cutaneous signs of NF1. However, it is important to consider that Lisch nodules are often undetectable in early childhood [4]. Lisch nodules are uncommon before 2 years of age and are only occasionally observed before 6 years of age. The prevalence, number, and dimensions of Lisch nodules are known to increase significantly with age [5]. In our study, Lisch nodules were found only in two eyes, in cases 3 and 5, at the initial visit. Lisch nodules newly appeared in two eyes in both cases 1 and 2 during the follow-up period. In case 5, the number of Lisch nodules increased from 2 to 3 after 5 years. These Lisch nodules were found only unilaterally in four of the five children with NF1, and in one child (case 4), no Lisch nodules had appeared by the final follow-up. These results are entirely consistent with the established facts that Lisch nodules are rarely detected at a young age and that their prevalence and number increase with age. The incidence of optic pathway gliomas ranges from 15% to 20% in NF1 patients [6], and in our case series, none of the patients were diagnosed with optic pathway glioma.
After the introduction of new ophthalmic imaging modalities, it became known that choroidal abnormalities are found in most NF1 patients. Yasunari et al. [7] reported a 100% prevalence of choroidal abnormalities in 17 NF1 patients. Viola et al. [8] published the largest cross-sectional study on this topic, which included 95 NF1 patients and 100 healthy control subjects; choroidal nodules were detected by NIR in 82% of the NF1 population, including 71% of a pediatric NF1 population aged 12 years or younger. The diagnostic accuracy was 90% in the overall population and 83% in the pediatric population [8]. Goktas et al. [9] reported a prevalence of 78.9% in a pediatric population of 19 patients aged 4 to 16 years. Parrozzani et al. [10] published the largest pediatric cohort study, which included 140 pediatric NF1 patients, 59 NF1-suspected patients and 42 healthy subjects; choroidal abnormalities were found in 60.5% of the affected and 2.4% of the suspected patients. Vagge et al. [11] reported nodules in 69.2% of 78 patients with a mean age of 8.1┬▒3.5 years. Cassiman et al. [12] reported nodules in 65% of 34 patients.
When NIR imaging and OCT scans were performed for our cohort, which included five Korean patients with NF1, choroidal nodules were found in all eyes. Among the studies published so far, a 100% prevalence of choroidal abnormalities in NF1 patients was reported only by Yasunari et al. [7], who evaluated 17 Japanese patients. These results show that the prevalence of choroidal abnormalities is significantly higher in Asian patients. Race might be one of the factors affecting the detection of choroid nodules using NIR imaging. This might be due to racial differences in choroidal melanin content [13]. In some cases reported in European countries, such as the one reported by Cassiman et al. [12], choroid nodules were visible in color fundus photography. However, no abnormalities were noted in color fundus photography in our cases or in the cases of Yasunari et al. [7]. These findings imply that NIR imaging and OCT scans are critical diagnostic tools for NF1 in Asian patients.
Slit-lamp examinations performed on the same day as that of the NIR imaging revealed that only four of the 10 eyes had Lisch nodules. This finding coincides with the previous report that the prevalence of choroidal nodules detected by NIR (71%) was much higher than that of Lisch nodules (43%) in pediatric NF1 patients [8], and implies that the choroid seems to be one of the most commonly affected tissues by NF1. A previous histologic study showed thickening of the posterior retina in NF1 patients, which was caused by a proliferation of neural-crest-derived melanocytes and neural cells in the choroid [14]. A high melanin concentration due to an increased number of neural-crest-derived melanocytes might induce strong backscattering to NIR lights, which in turn might enable choroidal nodules to be more visible in NIR imaging than in color fundus photography [15]. Spectral-domain OCT scans taken simultaneously with NIR imaging in an earlier study showed that choroidal abnormalities in NIR images were confined to the choroid [8].
NIR imaging is a valuable diagnostic method for pediatric NF1 patients because it is sufficiently sensitive to detect early-developed ocular signs and can be obtained in a short time without glare.
In cases 1 and 4, one of the choroidal nodules was located within the macular region. The BCVA of the affected eye was 20/25 in case 1 and 20/20 in case 5, which was the same as the opposite eye. This shows that the choroidal nodules did not affect vision. Further evaluation, such as a visual field test, might be helpful to support this conclusion.
Our study is limited by its small sample size, since only five patients were included. Furthermore, some of the examinations related to NF1, such as genetic tests, were not fully done in our clinic. However, these five patients fulfilled at least two of the clinical manifestations to be diagnosed as NF1.
In conclusion, choroidal nodules are a more common and earlier-detected ocular manifestation than Lisch nodules in Korean children with NF1. NIR imaging enables quick, reliable, non-invasive examinations of the choroid to detect choroidal abnormalities; as such, it may be useful for diagnosing NF1 in patients who are young and/or lack cooperation. Further, NIR imaging along with OCT can help to localize choroidal nodules in NF1 patients.