Characteristics of Functional Speech Sound Disorders in Korean Children
Article information

Abstract
Purpose
A speech sound disorder (SSD) is defined as the presence of a problem with articulation and phonological processes in a child. This study analyzed the clinical characteristics of Korean patients with functional SSDs without any neuromuscular abnormalities.
Methods
The medical records of patients aged 36 to 72 months old who were diagnosed with SSDs were retrospectively reviewed. SSD patients who scored less than 85 in the U-Tap test were divided into two groups according to their receptive language scores on the Preschool Receptive-Expressive Language Scale (PRES)/the Sequenced Language Scale for Infants (SELSI).
Results
Sixty-seven percent of patients with language impairment (LI) who were diagnosed with an SSD initially visited the hospital for a delay in language development (n=18, 66.7%). Among children with only an SSD, 26.7% (n=8) of the patients recognized it as a language developmental problem. All SSD patients had substitution errors in the onset of initial syllables (SSD, SSD+LI: 100%; typical development [TD]: 37.5%). Of particular note, SSD children with LI had more omission errors (55.6%) than patients with SSD only (16.7%). SSD patients had higher error rates than TD children in all consonants except for the glottal element (P<0.01). The lower the U-Tap score of SSD patients, the lower their expressive language score (P<0.001).
Conclusion
A high percentage of children with SSD initially visited the hospital for the treatment of language development delays. Articulation tests are essential for children who suffer from language delay. Furthermore, since incorrect articulation can lead to delays in expressive language development, early interventions should be considered.
Introduction
Inaccurate pronunciation is attributable to disorders of central and/or peripheral origin (articulation vs. phonologic disorders, respectively). Distinguishing between these types of disorders is challenging. The inability to correctly pronounce certain speech sounds beyond the age at which the sounds are usually learned (caused by an articulation or phonological disorder) is referred to as a speech sound disorder (SSD) [1,2]. A Korean syllable consists of an onset, nucleus, and coda. A child who is unable to correctly pronounce any of these phonemes is considered to have difficulty with sound production. SSDs occur secondarily to functional or symptomatic etiologies. Symptomatic etiologies include underlying neurological, structural, or sensory causes. Nonetheless, the exact etiologic contributors to functional SSDs remain unknown. Children with functional disorders may show improved pronunciation with age; however, some children show persistent pronunciation impairment [3,4]. Children with persistent articulation impairment may show poor language-related skills, including reading and literacy ability and perception [5-7].
A child’s speech-production skills develop during the cooing and babbling stages. Children usually attain phonological characteristics similar to those of adults by 3 to 5 years of age. A majority of Korean children can use most syllable structures proficiently by 4 years of age [8]. In a study published in 1996, the authors scored the accuracy of consonants used by Korean-speaking children between 2 and 6 years of age based on the degree of errors of substitution, distortion, and omission [9] and observed that pronunciation of the /s/-series appeared at 2 to 3 years of age, although satisfactorily accurate pronunciation was observed only by 6 to 7 years of age [9]. A cross-linguistic review across 31 countries and 27 languages, including Korean, reported that 5-year-old children could accurately pronounce at least 93% of consonants [10]. However, large-scale studies from English-speaking countries have shown that 3% of the children investigated did not acquire adequate consonant pronunciation skills at 4 years of age [11]. Various studies have reported the SSD prevalence in children between 5 and 8 years of age to be 3.8%–6.4% [12-14]. Regardless of the language, SSDs in preschool-aged children usually significantly affect articulation and literacy outcomes in later years, and the outcomes may be poorer depending on the error pattern [3,15]. Notably, poorer outcomes are reinforced in children with concomitant language impairment (LI) [11,16]. Therefore, a thorough understanding of the error patterns and accompanying language underdevelopment in preschool-aged children with SSDs is important for predicting their prognosis and initiating early interventions.
A Korean study reported that 2.5% of children had SSDs and 6.4% were at risk; however, the study lacked descriptions of the characteristics of SSDs in Korean-speaking children [17]. In Korea, SSDs are usually diagnosed based on the following tests: the Urimal Test of Articulation and Phonation (U-Tap), the Korean Standard Picture Articulation and Phonology test, and the Assessment of Phonology and Articulation for Children test [18]. We selected the U-Tap test as the evaluation tool for SSD diagnoses because the U-Tap is the most widely accepted articulation/phonology test in the field. Language development measurements were performed using the Preschool Receptive-Expressive Language Scale (PRES) and/or the Sequenced Language Scale for Infants (SELSI) based on the child’s age.
In this study, we investigated the clinical characteristics of Korean patients with functional SSDs. We excluded patients with neuromuscular abnormalities or abnormalities detected on brain magnetic resonance imaging (MRI). We specifically focused on differences based on the degree of LI and in comparison with children who showed typical development (TD).
Materials and Methods
1. Subjects
We analyzed data of children aged 36 to 72 months, who underwent language tests at Jeonbuk National University Children’s Hospital between January 2016 and December 2020. The total number of participants was 974, of whom 410 were excluded because they had neuromuscular disorders (such as epilepsy or cerebral palsy), or electroencephalography- or brain MRI-documented abnormalities that may affect speech and language ability. We also excluded patients with tongue or oral cavity abnormalities. We defined an SSD as a U-Tap score <85 (below –1 standard deviation). Since the U-Tap score was low owing to a lack of language development, and not articulation impairment, in such cases, we excluded patients in whom the PRES score was not higher than the U-Tap score by 10 points or more. Finally, 57 patients were included in the study.
All children underwent the U-Tap test for pronunciation and PRES or SELSI screening to evaluate language development [19]. The PRES measures the receptive and expressive language abilities of preschool-aged children between 2 and 6 years of age and expresses the score as a percentage by dividing the developmental age obtained through the test by the actual age. The SELSI is used to evaluate language ability in children between 5 and 36 months of age, as well as in children with delayed language development. Overall, the PRES screening test was administered more frequently than the SELSI in children between 3 and 6 years of age; however, the SELSI was more commonly used in children with significantly delayed language development [20]. Based on language tests, children with a developmental quotient ≥85 were deemed to have normal scores.
The U-Tap includes a total of 43 consonant tests (18 in the syllable onset, 18 in the nucleus, and seven in the coda). The score is expressed as a percentage of consonants that are correctly pronounced [21]. The 18 consonants can be classified into the following eight subtypes: [p/b,p*,ph] are classified as bilabial plosives, [m,n] as nasal, [h] as glottal, [k/g,k*,kh]/ as velar plosives, [t/d,t*,th]/ as alveolar plosives, [s,s*] as alveolar fricatives, [ʧ, ʤ,ʧ*,ʧh] as palatal affricates, and [l/r] as a liquid. The U-Tap test was performed in the context of words and sentences. Incorrect pronunciations of consonants were marked on the checklist, and the errors were categorized into substitution, distortion, or omission errors. For example, if /사탕/ satang [sɑ:tǽŋ] (meaning ‘candy’ in Korean) was pronounced as /다탕/ datang [dɑ:tǽŋ], it was classified as a substitution error. If it was pronounced as /thatang/ [ðɑ:tǽŋ], the error was categorized as distortion because /th/ [ð] is not a component of the Korean phonological system, and if it was pronounced as /아탕/atang [ɑ:tǽŋ], the error was categorized as omission. Based on their receptive language scores obtained after PRES/SELSI testing, patients with SSDs were categorized into two groups. Children with scores <85 for receptive language were classified into the SSD+LI group and those with scores ≥85 were classified into the pure SSD group. Children in whom both tests showed scores within the normal range were included in the TD group, which was compared with the SSD group.
2. Clinical factors
We investigated various clinical characteristics, such as the patient’s chief complaint, sex, age, gestational age at birth, birth weight, mode of delivery, number of siblings, duration of breastfeeding, head circumference, mean video or cellular phone exposure time per day, the timing of first word expression, and attention deficit-hyperactivity disorder, as predictor of language function in children. We compared clinical characteristics between the SSD and SSD+LI groups and TD group. We evaluated factors that affect U-Tap scores regardless of language ability. Differences in vulnerable consonants were also compared and analyzed. This study was approved by the Institutional Review Board (IRB) of Jeonbuk National University Hospital (IRB No.2021-05-053). Written informed consent by the patients was waived due to a retrospective nature of our study.
3. Statistical analysis
Clinical characteristics were summarized using means, standard deviations, and percentages. One-way analysis of variance, the Kruskal-Wallis test, and the chi-square test were used to compare differences in characteristics and U-Tap scores between the two SSD groups and the TD group. Multiple logistic regression analysis was performed to identify correlations between clinical characteristics and the U-Tap score. We performed the chi-square and Fisher exact tests to assess the significance of differences in the frequency of consonant errors among the three groups. All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
Results
1. Clinical characteristics of patients with SSD
Table 1 shows the characteristics of the 57 participants with SSDs and the 16 participants with TD. Both SSD groups included a high percentage of male patients (SSD: 80%; SSD+LI: 66.7%), and the mean patient age in the SSD groups was 45.3±8.7 and 46.4±7.7 months, respectively. We observed no significant differences in sex and age between the SSD and TD groups. There was a tendency for children with SSD+LI to have been evaluated at other hospitals, where they were shown to have abnormalities on the Korean Developmental Screening Test for infants and children (K-DST) (51.9%), whereas in most children with pure SSDs (56.7%), parents first observed the articulation difficulties. Two-thirds (66.7%) of patients with language delay were diagnosed with SSDs incidentally during hospital visits for the evaluation of delayed language development. Children with pure SSDs were usually evaluated for pronunciation disorders; however, 26.7% of patients considered this to be LI. The children in the SSD+LI group spent significantly more time watching TV than those in the other groups (P<0.01). We observed no significant intergroup differences in other clinical characteristics.
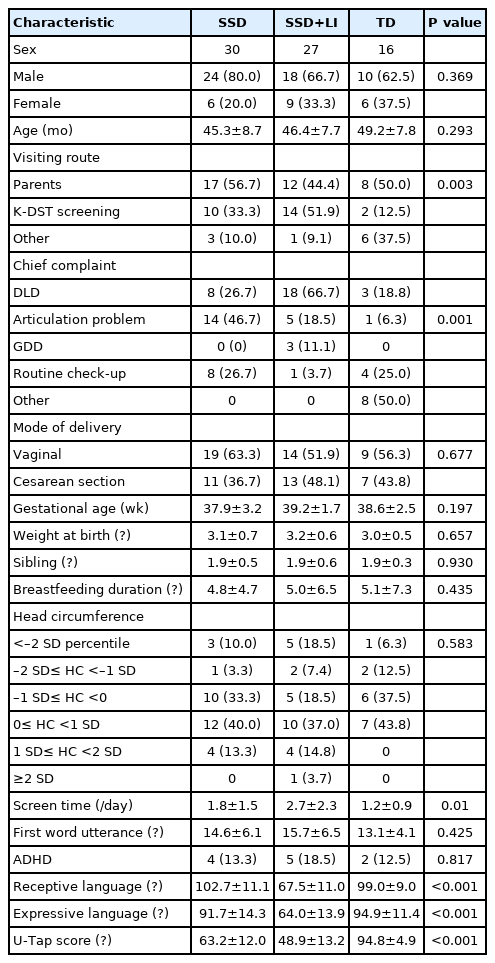
Clinical characteristics of SSD patients
2. Comparison of consonant error patterns between children with SSDs and those with TD
We quantified cases in which children had substitution, distortion, or omission errors in the 43 consonant tests. All patients with SSDs had substitution errors in the initial syllable onset position (SSD and SSD+LI: 100%; TD: 37.5%) (Fig. 1A). Typically, the SSD+LI children also had many omission errors (55.6%), unlike the findings in patients with pure SSD (16.7%). Notably, no child with TD showed an omission error in the first syllable. These error patterns are similar to those depicted in Fig. 1B, which shows errors in the onset elements in the middle of words. All patients with pure SSD and SSD+LI had substitution errors; specifically, children with SSD+LI had high rates of omission errors (SSD: 53.3%; SSD+LI: 88.9%). Fig. 1C and D show the error probability for each consonant group regardless of the error type. Overall, children in the TD group showed nearly no errors in bilabial, nasal, and velar plosives, whereas a significantly higher percentage of children with SSD had onset errors in the initial syllable. For example, only 6.3% of children in the TD group had incorrect pronunciation of the bilabial sound in the initial syllable, whereas we observed significantly higher rates of errors in the pure SSD (23.3%) and SSD+LI (51.9%) groups (Fig. 1C). No children in the TD group showed articulation errors with regard to nasal and liquid sounds, whereas significantly higher rates of errors were observed in the SSD groups (nasal [SSD, 23.3%; SSD+LI, 51.9%], liquid [SSD, 66.7%; SSD+LI, 70.5%]). Errors in bilabial, nasal, and liquid sounds even in the middle of the word were significantly more common in the SSD group than in the TD group (Fig. 1D). All three groups showed few error rates for the glottal phoneme. These results indicate that the patients with SSDs experienced significant difficulty with the pronunciation of even relatively easy sounds.
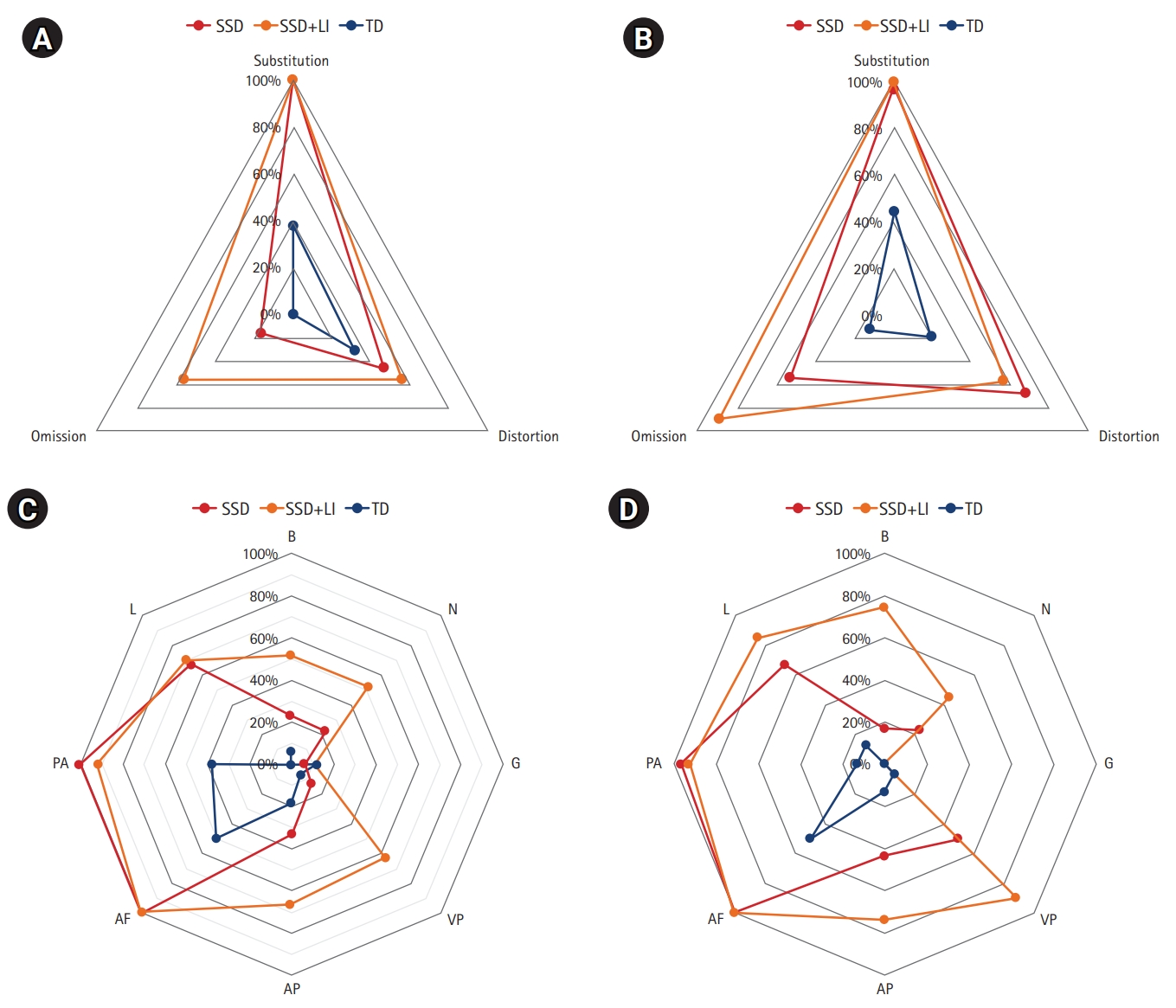
Distribution of proportions of errors according to type and consonant category in children with typical development (TD), speech-sound disorders (SSD), and SSD+language impairment (LI). (A) It is the onset error of initial syllable and (B) is the error of the middle of words on all SSD patients, (C) and (D) show the error probability for each consonant group regardless of the error type. B, bilabial; N, nasal; G, glottal; VP, velar plosive; AP, alveolar plosive; AF, alveolar fricative; PA, palatal affricate; L, liquid.
Comparable results were obtained in a data analysis based on consonant phonemes and error types (Table 2). The SSD group showed significantly higher substitution error rates at both the beginning and middle of words (P<0.01). Omission errors were significantly more common in the SSD+LI group than in the pure SSD group with regard to bilabial, nasal, velar plosive, alveolar plosive, palatal affricate, and liquid sounds (P<0.01). With regard to the error patterns of total consonants, the error rates in all consonants except for the glottal element were significantly higher in the SSD groups than in the TD group (P<0.01). This trend was statistically more significant with regard to the alveolar fricative, palatal affricate, and liquid consonants (P<0.001).
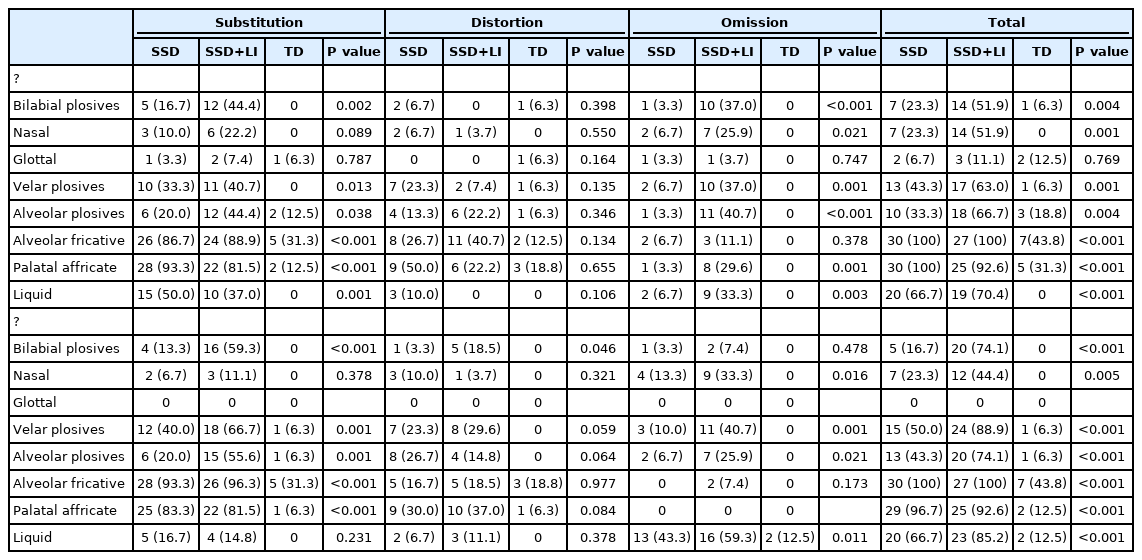
Statistical differences of consonant errors in SSD patients and TD children
3. Associations between the U-Tap score and clinical characteristics
We investigated the clinical characteristics that were likely to be associated with the U-Tap score (Table 3). Age and expressive language function showed significant correlations with articulation. Specifically, younger age was associated with lower U-Tap scores (P=0.016). Additionally, a low expressive language score was associated with poorer articulation (P=0.001). Sex, mode of delivery, gestational age, birth weight, and mean time spent watching movies did not affect the acquisition of articulation skills (P>0.05).

Correlations between clinical factors and the U-Tap score (P values)
Discussion
In this study performed in Korean preschool-aged children, we compared consonant errors between children with SSD and those with TD. SSD was commonly observed in boys (SSD: 80.0%; SSD+LI: 66.7%) (Table 1). This finding is consistent with the results of previous studies, which have reported that preschool to early-school girls tend to show better speech intelligibility, clarity of articulation, and fluency [22-24]. The mean age of patients with SSDs was 45 to 46 months. Several studies have reported that speech intelligibility may improve with age; accuracy was shown to increase from 26% to 50% by 2 years of age and to nearly 100% by 4 years of age [25-27]. Although most children between 3 and 5 years of age show complete consonant acquisition, children with pure SSDs showed a poor U-Tap score of 63.2 at this age, while those with SSD+LI had a score of 48.9, suggesting that these children have a true articulation disorder and not immature pronunciation attributable to young age. These children usually present to the hospital for an evaluation of delayed language development or articulation difficulties. We observed that 14 of the 30 patients with pure SSDs (46.7%) were aware of their speech impairment, whereas eight (26.7%) children perceived this disorder as a language developmental delay. Furthermore, only 18.5% of the patients with SSD+LI were aware of the accompanying inaccurate pronunciation. Therefore, articulation screening tests are important for children with delayed language development. We observed no difference between the pure SSD and TD groups with regard to the time spent watching videos. However, children with SSD+LI spent significantly more time watching TV/videos than those with pure SSDs (P=0.01), suggesting that watching videos had a negative effect on language development.
Overall, compared with the TD children, those with SSDs experienced difficulties with most consonants, except the glottal element (Table 2 and Fig. 1). Almost all (90% to 100%) of children with SSDs did not correctly pronounce difficult consonants such as the alveolar fricatives and palatal affricates, which are frequently associated with errors even in normal preschool-aged children. These results are similar to those of a previous study that described types of consonant errors in Korean-speaking children between the ages of 3 and 5 years, in which the authors observed that speech sound errors were the most frequent in the order of onset-fricative, nucleus-fricative, and onset-liquid [28]. In English, the easy pronunciation of /m/, /n/, /h/, and /w/, among others is completed first, and alveolar fricatives such as /s/, /sh/, /ch/, /th/, /z/ and liquids (/l/ and /r/) develop later [29,30]. Therefore, researchers have concluded that the maturation of fricative-related pronunciation is slower, and comparisons between children with SSDs and TD may show similar tendencies regardless of the language. SSDs are associated with frequent errors even in the pronunciation of easy consonants. Children with TD showed nearly no errors with regard to the bilabial plosives, nasals, velar plosives, and alveolar plosives, whereas those with SSD and SSD+LI showed a significantly higher error rate. Most errors in the pure SSD group were of substitution, whereas children with SSD+LI showed both omission and substitution errors. Similar findings were observed in a Spanish study performed by Bosch and Serra, who observed an overall higher incidence of omission than substitution errors in monolingual Spanish-speaking children with LI [31]. Several studies that have investigated pronunciation errors in Spanish-speaking children with LI have reported that omission errors were more common than substitution errors [32,33]. In contrast, substitution errors were more frequent in English-speaking children with LI [34,35]. It is reasonable to conclude that these error patterns tend to vary with language. In our study, we observed a higher prevalence of omission errors in Korean-speaking children with LI.
Clinical characteristics such as birth weight, mode of delivery, duration of breastfeeding, siblings, and head circumference did not affect the U-Tap score (Table 3). However, age and expressive language scores (P=0.001) obtained on PRES testing were correlated with the U-Tap score (P=0.016). Low U-Tap scores were associated with low expressive language scores. We observed no correlation between the U-Tap score and receptive language ability. These results suggest that inaccurate articulation is not merely a simple pronunciation difficulty, but a disorder that can significantly affect a child’s expressive language skills.
The clinical implications of these findings are as follows. (1) Many children diagnosed with SSDs initially sought medical attention for evaluation of delayed language development. Articulation tests are indicated in children who present with a major complaint of language delay. (2) Children with SSDs may occasionally present with concomitant expressive language delay; an early and accurate diagnosis and prompt initiation of treatment are necessary in such cases. (3) Children with SSDs tend to struggle even with pronunciation of easy consonants, and those with accompanying LI show a greater variety of errors than children with pure SSDs or TD. Therefore, both language function and articulation/phonological tests should be performed in all children with pronunciation problems and/or developmental language delays.
The limitations of this study are as follows. (1) We enrolled a limited number of preschool-aged children with SSDs; therefore, the small sample size is a drawback of this research. (2) A single language test was used in this study, and our results might not be generalizable across different languages. Large-scale studies are warranted in the future to investigate changes in expressive language function based on post-treatment improvement in articulation and prognosis in school-aged children.
Notes
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: SJK. Data curation: MJH. Formal analysis: MJH. Methodology: MJH and SJK. Project administration: SJK. Visualization: MJH and SJK. Writing-original draft: MJH. Writing-review & editing: SJK.