The Mini-Mental State Examination (MMSE) as a Cognitive Screening Tool in Duchenne Muscular Dystrophy
Article information

Abstract
Purpose
Given that intellectual disability affects 15% to 63% of boys with Duchenne muscular dystrophy (DMD), it is relevant to evaluate if the Mini-Mental State Examination (MMSE) is a reliable test for screening in these cognitively impaired boys.
Methods
A descriptive study of 74 DMD boys was performed. Age, years of schooling, genotype, and performance in the MMSE and Wechsler Intelligence Scale for Children (WISC)-IV were verified.
Results
Sixty-seven patients, with a mean of age 12.1±3 years were enrolled. Verbal comprehension (76.9±13.9) and working memory (71.2±16.7) indexes showed the highest impairment. Correlation between the MMSE (20.3±6.1) and WISC-IV (74.4±15.6) was moderate (r=0.556).
Conclusion
The MMSE is a good cognitive screening test for DMD patients of 9 years and older, particularly in countries where the public health system does not provide expensive neuropsychological batteries, and has 78% accuracy and 82% sensitivity for scores ≤21. Subtests of the MMSE with better discriminatory power (for orientation, attention, and calculation) can help educators, teachers, and families to develop simple activities or academic games that enhance such mental skills.
Introduction
Duchenne muscular dystrophy (DMD), a lethal X-linked recessive neuromuscular disorder, is caused by mutations in the gene encoding the dystrophin protein. Besides muscle weakness, static cognitive and language disabilities are also present. Point prevalence per 100,000 males varies from 1.9 (2012) in the USA to 6.1 (2012) in Canada [1]. Higher rates of intellectual disabilities (ID), ranging from 15% to 65%, are reported among DMD patients [2].
Clinical literature reports a high rate of ID (ranging from 15% to 63%) [2-12], borderline intelligence (10% to 26%) [6-8], mild ID (15% to 27%) [2,6,10,11], moderate ID (6.7% to 10%) [2,10], severe ID (0.4% to 10%) [2,10], and profound ID (0.08%) among DMD patients [2]. Several studies have found an overall reduction of intelligence quotient (IQ) in boys with DMD, by the Wechsler scale, recording total scores from 76 to 90.2 [2-7,9,13-15].
The DMD gene contains 79 exons and seven alternative promoters, that generate different protein isoforms with diverse tissue expression patterns. The exact role of dystrophin isoforms in the central nervous system remains unclear; however, it is possible that mutations affecting Dp140 [4-8,11,14,16-18] and Dp71 [5-7,8,11,14,19-22]. DMD patients without Dp140 show reduced gray matter volume and decreased cerebral blood flow [23,24]. The absence of dystrophin has been established to result in aberrant synapse maturation and neurotransmission in the hippocampus, neocortex, cerebellum, and amygdala, and has been linked to learning and memory problems [25].
Several precise and complex cognitive batteries, such as Wechsler Intelligence Scale for Children (WISC), are available to appraise developmental and intelligence deficits in childhood, but they require specific training for the examiner, are expansive and have long testing time. The Mini-Mental State Exam (MMSE) is an easy, quick and reliable test for cognitive screening in adults, which can be carried out in 5 minutes [26]. Some authors have performed several modifications to the original MMSE for use in young children [27-29]. Only one study evaluated the original MMSE in 181 healthy children (4 to 12 years), and scores surpassed 24 points, on average, at the age of 6, which is considered the cutoff to distinguish healthy adults from those cognitively impaired [30] Modified versions of the MMSE in childhood have shown correlations with WISC, and can be used as a screening tool for detection of learning disabilities. The Brazilian researchers evaluated 103 children (6 to 9 years) with learning disabilities. The Italian study has been shaped MMSE in three different versions according to school class in children aged 6 to 13 [31,32]. Original MMSE or modified versions of MMSE has not been explored in other specific neurological diseases in childhood.
Besides neurodevelopmental evaluation and school history review is part of a standard medical consultation, it is important to provide an objective cognitive measure close to the literacy age in boys with DMD. Although a simple cognitive screening test such as MMSE does not replace neuropsychological evaluation, their application can be cost-effective in the Brazilian public health system with narrow budget. It is important to verify the applicability of the original MMSE in this group, which could demonstrate early handicaps, and possibly guide the appropriate pedagogical counseling and the speech therapy intervention. Our aim was to verify the potential use of the MMSE as a cognitive screening tool in a group of boys with DMD comparing it to the WISC rates and describe the genotypes in this convenience sample.
Materials and Methods
1. Participants
A primary observational, cross-sectional, prospective, and descriptive study of 74 boys with DMD was performed. All patients were recruited as a convenience sample from a public outpatient clinic of low socioeconomic and educational status in Rio de Janeiro, Brazil. The study protocol was approved by the Ethics Committee of Puericultura and Pediatria Martagão Gesteira Institute (IPPMG)/Federal University of Rio de Janeiro (UFRJ) (CAAE number: 43450415.0.0000.5264). Informed written consent was obtained from parents. The inclusion criteria were (1) diagnostic confirmation of DMD by genetic testing (polymerase chain reaction, multiplex ligation-dependent probe amplification, or exome sequencing) and/or by identification of typical histopathological changes from muscle biopsy; (2) age from 6 to 16 years old; and (3) minimum length of schooling 3 years. The exclusion criteria were (1) selective mutism; (2) previous medical history of central nervous system injury (hypoxic-ischemic event, premature birth, neonatal jaundice, neonatal sepsis, congenital hypothyroidism, drugs, or alcohol consumption during pregnancy), severe psychiatric disorder or any sensory deficit that could interfere with the execution of the test; (3) non-invasive or invasive ventilation support with inability to speak and answer oral questions; and (4) muscle strength grading 0 or 1 in the distal upper limbs, impairing writing or drawing.
2. Procedure
Neuropsychological tests consisted of the MMSE Brazilian version [33] as a screening test for ID, and the WISC Fourth Edition (WISC-IV) Brazilian version [34] as the gold-standard for stratification of IQ. This scale is divided into four indexes that contribute to a total full scale of IQ (FSIQ): verbal comprehension index (VCI), an overall measure of verbal concept formation; perceptual reasoning index (PRI) a measure of non-verbal and fluid reasoning; processing speed index (PSI), a measure of visuo-motor integration; and learning and working memory index (WMI), a measure of memory span and freedom from distractibility. According to WISC-IV, patients were divided into four categories based on their IQ scores: normal intelligence (80 to 119), borderline intelligence (70 to 79), mild ID (55 to 69), and moderate ID (40 to 54) [34]. The definition of ID was also based on the diagnostic and statistical manual of mental disorders 5 (DMS-5) clinical criteria: (1) deficit in intellectual functions and (2) deficits in adaptive functioning (conceptual, social, and practical domains) [35].
Cognitive tests were administrated during regular medical visits in different rooms and by the same medical researcher (MMSE) and neuropsychologist (WISC-IV). The total time taken for the administration of the MMSE was around 5 minutes and the WISC-IV lasted 50 minutes. Sociodemographic data (age, patients’ years of schooling, mothers’ years of schooling, fathers’ years of schooling) and genetic profile (type and site of genetic mutations) were registered during interview and/or from medical records. The sample was also subgrouped on the basis of genetic mutation site, as those with mutations upstream of exon 30 (proximal mutations), between exon 31 and 62 (middle mutations disrupting Dp140), or downstream of exon 63 (distal mutations disrupting Dp71).
3. Data analyses
Microsoft Excel electronic worksheets for Mac 2011 version 14.7.2 and the SPSS Statistics version 20.0 (IBM Co., Armonk, NY, USA) for Mac 2011 were used to plot the data and for statistical analyses. We first undertook descriptive analysis of the sample distribution according to chronologic age, patient’s school grade (years of schooling), parents’ school grade (years of mother’s and father’s schooling) and type/site of genetic mutation. Measures of central tendency (mean, mode, median), standard deviation, and maximum and minimum values were calculated. Continuous variables with a normal distribution were analyzed with the Student’s t-test for independent samples; the Mann-Whitney U test was applied for variables with non-normal distribution, and statistical significance was set at P≤0.05. Spearman's correlation coefficient was used to assess the relationship between MMSE total score and other variables such as chronologic age, school grade, parents’ school grade, and WISC-IV test scores. Categorical variables were plotted in crosstabs and evaluated by chi-square test/Fisher’s exact and kappa concordance tests. The receiver operator characteristic (ROC) curve was calculated to reach the best MMSE cut-off point to adequately screen ID. Validity tests (sensitivity, specificity, positive/negative predictive value and positive/negative likelihood ratio) were implemented for different MMSE cut-off points, in order to define which had the highest accuracy.
Results
1. Patient sociodemographics
Of the 74 DMD patients regularly followed in our center during the period of study, only 67 fulfilled all the inclusion criteria and the age range was between 6 and 16 years (mean 12.1±3 [range, 7 to 16]). Seven DMD patients were not included in the analysis, among which two had selective mutism, two had suffered neonatal hypoxia and three patients had hand muscle strength grading zero. The patient ages followed a normal distribution. Three patients were excluded because of selective mutism and four were out of age range. Fifty-three patients (74.6%) had a diagnosis of DMD through genetic testing, and 18 patients (25.4%) were diagnosed through muscle biopsy. The majority of mutations were intragenic deletions (50.7%). Single or multi-exon duplications accounted for 9.9% of patients, and point mutations accounted for 14.1%. Upstream exon 30 mutations (exons 1–30), middle mutations (exons 31–62) disrupting the Dp140 isoform, and downstream of exon 63 mutations (exon 63–79) disrupting Dp71, were seen in 28.2%, 35.2%, and 2.8%, respectively. The WISC-IV battery, used to grade cognitive categories, was applied in 53 patients only, due to staffing constraints. The FSIQ in the sample (53/67 patients) was 74.4±15.6, one standard deviation below the population mean (t-test one sample P<0.001). The VCI and WMI showed the highest impairment, with means scores of 76.9±13.9 and 71.2±16.7), respectively. The MMSE total mean score was 20.3±6.1 points in the DMD sample (t-test one sample P<0.001). On examining DMD patients without ID, we found cognitive performances belonging to the middle-lower stratum of the general population: FSIQ mean of 84.2±11.3), VCI mean of 84.1±12.1, and WMO mean of 80.4±13.1. Other descriptive information concerning sociodemographic data, MMSE total scores, WISC-IV total scores and index scores compared between the two groups (with and without ID), are shown in Table 1.

MMSE and WISC-IV total scores and indexes in Duchenne muscular dystrophy patients with and without ID
2. Neurocognitive profile
Nineteen of 53 patients showed normal IQ (28%), 13 patients borderline IQ (19%), 17 mild ID (25%), and four moderate ID (6%). None achieved a higher IQ or had severe/profound ID. Mean scores of MMSE and subtests are shown in Table 2. The MMSE total score increased with chronological age in both groups, with ID (rs=0.551) and without ID (rs=0.565), and with years of schooling (rs=0.437) (P<0.05). Correlation between MMSE and WISC-IV was positive and moderate (rs=0.556) and a similar trend in each of the four categories was observed (rs=–0.522) (P<0.05) (Table 3). The relationship between MMSE total score and age in DMD patients without ID is shown in Fig. 1. It can be seen that from 9 to 10 years of age the MMSE score reaches a stability plateau, and most scores are above 24 points, the cutoff value for healthy adults. Neuropsychological evaluation by MMSE and WISC-IV demonstrated the lowest scores in middle and distal mutations, although without statistical significance (Table 4).

MMSE and subtest in IQ stratification

MMSE and correlation with age (yr), patient's years of schooling and WISC-IV
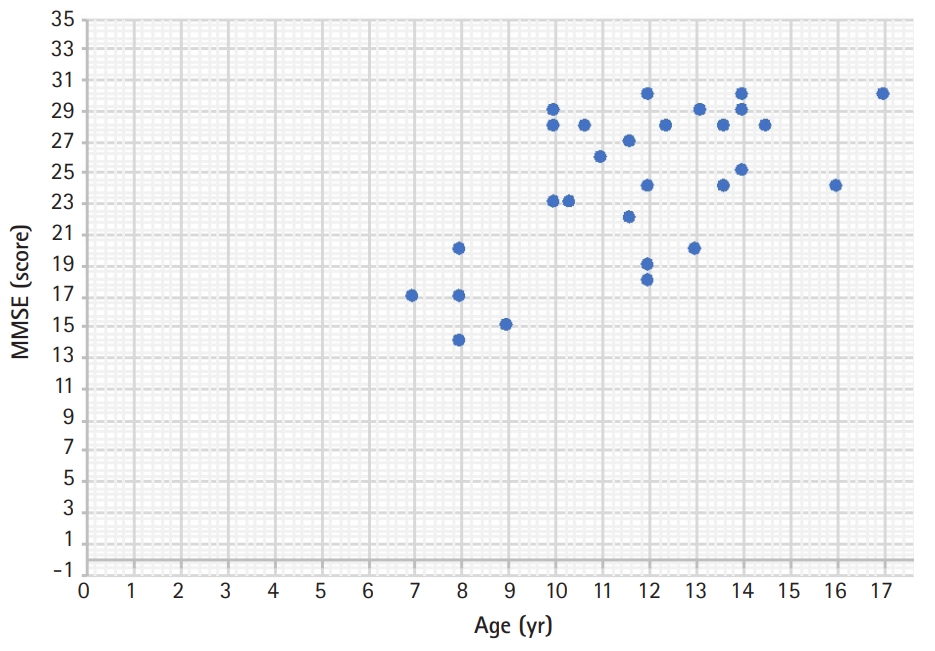
Correlation between Mini-Mental State Examination (MMSE) total score and ages in Duchenne muscular dystrophy patients without intellectual disability.

Correlation with neurocognitive phenotype and genotype
3. Validity of MMSE as a screening instrument for ID in DMD patients
The ROC curve for MMSE was drawn considering the clinical criteria of DSM-5 and/or WISC-IV score for ID diagnosis. The area under the ROC curve demonstrates 0.841 accuracy and the best cut-off points were 20, 21, and 22 (Fig. 2). Table 5 shows statistical analyses of validity measures for these set points. An MMSE score equal to, or below, 21 had 82% sensitivity, 74% specificity, and 78% accuracy, with a kappa coefficient of 0.567.
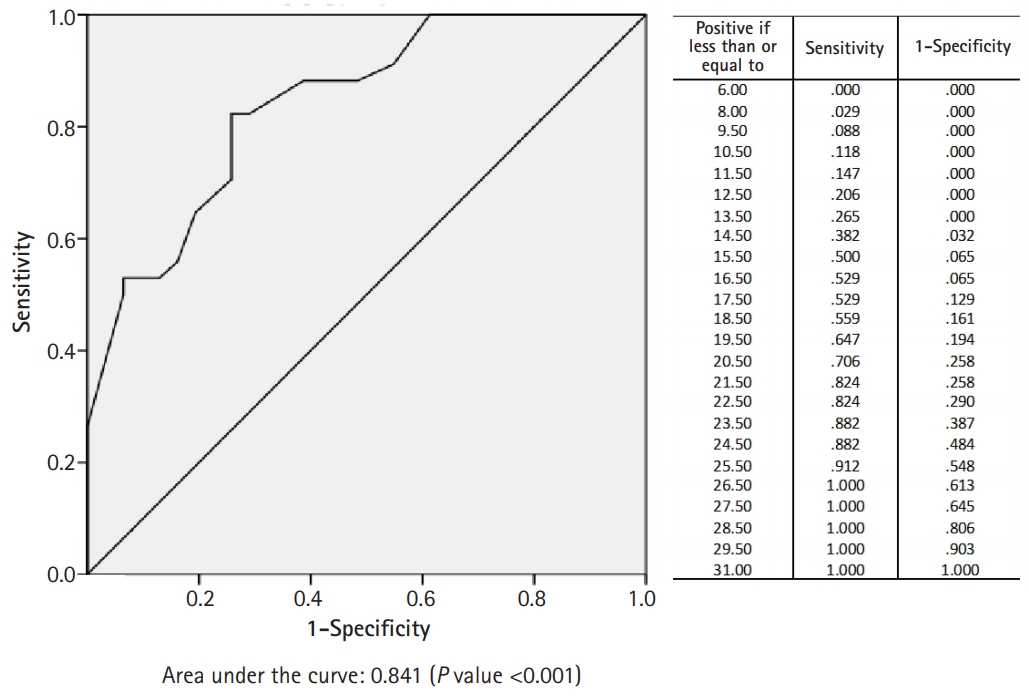
Receiver operator characteristic curve for Mini-Mental State Examination to screen intellectual disability in Duchenne muscular dystrophy patients.

Analysis of validity for cut-off points in MMSE to screen intellectual disability in Duchenne muscular dystrophy patients
Discussion
There is a growing interest in the neurobehavioral aspects of DMD, but data of using MMSE in this population is limited. We found that an MMSE score below 21 is a good ID screening test in boys with DMD, with 82% sensitivity, 74% specificity, and 78% accuracy. It can be seen that from 9 to 10 years of age, MMSE scores reach a stable plateau. Thus, the MMSE can be applied with reliability from 9 years of age in boys with DMD, because there is no further increase in score depending on age, maturation or experience.
The MMSE is a very important tool for the Brazilian child neurologist, allowing us to objectively measure higher mental functions, in addition to the usual neurodevelopmental assessments and review of school history. Overall, the MMSE proved to be a safe, easy, quick, and reliable tool, fulfilling the requirements of many public health systems that do not provide neuropsychological assessment to the population. Quantitative assessments can also reinforce academic, pedagogical, and speech-language stimulation therapies, as well as improve treatment adherence. In Brazil, children are admitted to school at the age of 6 years, and a cognitive screening at age 9 years would greatly improve health and educational policies for ID in DMD.
In 2018, our team published preliminary data from an observational and descriptive study of 34 boys with DMD followed in our center, aged between 8 and 22 years, in whom an exploratory analysis was performed. We assessed MMSE, developmental milestones, independence in daily life activities, and literacy skills. In this previous study, the MMSE was not compared to any gold-standard neuropsychological test, and ID diagnosis was based on DSM-5 clinical criteria. The most accurate cutoff value on the MMSE to distinguish moderate-severe ID in DMD patients was 21 (P<0.005). This proved that the MMSE is a reliable test for detection of ID, even in small samples [36].
Our results confirm some cognitive aspects in DMD patients. We found a higher rate of ID (52%) in our sample, probably due to intrinsic genetic background and unfavorable social environment. Parents’ academic graduation, especially the father's years of schooling, were lower in DMD patients with ID (mean 8.3±3.9) than in DMD patients without ID (mean 11.5±4.5; P<0.05). The FSIQ mean score (74.4±15.6) was one standard deviation below the normal population, with obvious performance impairment in two items: verbal skills (VCI mean 76.9±13.9) and working memory (WMI mean 71.2±16.7). This Brazilian neuropsychological profile is worse than previously reported in the scientific literature, and we suppose that lower socioeconomic and educational background in this group contributed to these results [2-7,9,13-15]. Higher mental functions that are dependent on working memory, like attention and concentration, were also the most impaired in DMD patients without ID and the mean WMI was 80.4±13 (P<0.05). This score belongs to the middle-lower range of IQ in the general population. Aside, the WMI score in our study was lower than the average found by Battini et al. [12] (WMI 88.5±17.4), supporting that executive functions are disabled in all DMD patients, even with normal IQ.
The mean MMSE total score was 20.3±6.1, and in patients with ID (16.9±5.2) it was significantly lower than in patients without ID (24.1±4.6), considering groups with similar mean chronological age (12.2 years vs. 11.5 years) and years of schooling (6.6 years vs. 6.8 years). At the age of 9 to 10 years in the group without ID, MMSE scores exceeded 24 on average. Healthy children reach 24 points on the MMSE at the age of 6 years [30], showing that even DMD patients without ID are slow to achieve this set point when compared with their peers. The greatest shortcoming of MMSE, predictable by the lack of refinement of its items, lies in its inability to detect borderline IQ and other learning disorders, which are known to affect DMD patients without ID. This current study, none additional neuropsychiatric diagnosis (autism spectrum disorder, attention deficit and hyperactivity disorder, specific learning disorders).
The total MMSE score correlated moderately with the child’s chronologic age (rs=0.55, P<0.001), years of schooling (rs=0.43, P<0,001), and WISC-IV score (rs=0.55, P<0.001). Rubial-Alvarez et al. [30] found a stronger correlation with chronologic age (rs=0.8, P<0.001) and mental age (rs=0.76, P<0.001) in healthy children aged between 4 and 12 years, but they did not evaluate boys with DMD [30]. Some authors used a modified MMSE version, instead of the original one for healthy children, and therefore their results should not be compared with our data [27,28,31,32].
Cognitive stratification based on IQ showed a similar distribution to that in the literature: 28% (normal IQ), 19% (borderline intelligence), 25% (mild ID), and 6% (moderate ID). Severe ID and profound ID has been estimated in 0.4% to 10% and 0.08% of patients [2-10], but we did not find these categories in our sample. There was a clear decreasing gradient of mean MMSE total score in four cognitive categories: 24±4.9 (normal IQ), 23.1±4.5 (borderline IQ), 18.6±6 (mild ID), and 12.5 (moderate ID) (rs=0.52, P<0.001). Subtests of MMSE with better discriminatory power among cognitive categories were orientation (rs=–0.49, P<0.001), attention and calculation (rs=–0.46, P=0.001). Language subtest, despite statistical significance, did not demonstrate clinical differences among cognitive categories, because mean scores were very close to each other. According to the moderately positive correlations between the MMSE and WISC-IV, and the area under the ROC curve (0.841), validity measures were also explored. We showed that a score under or equal to 21 in the MMSE had the best sensitivity (82%), specificity (74%), positive predictive value (77%), accuracy (78%), and kappa concordance (0.567) for screening of ID in DMD patients. de Souza Moreira et al. [37] assessed 54 children and adolescents with learning disabilities in Brazil, comparing the adapted pediatric version of the MMSE and WISC-IV. They found a score of 18 is the best cut-off point to screen ID (sensitivity 55%, specificity 64%, and accuracy 59%) [37]. We believe that adapted pediatric versions of the MMSE have easier tasks, which diminishes their discriminatory power.
Genetic mutation affecting exons 31–62 (disrupting Dp140) and exons 63–79 (disrupting Dp71) had a trend of lower average scores in both the MMSE (18.2±7 and 12.5±0.7, respectively) and WISC-IV (72.7±15.9 and 50.5±2.1, respectively), when compared with proximal genetic mutations (MMSE 22.2±3.8 and WISC-IV 76.4±24.4). ID was more commonly found in patients with middle mutations/exons 31–62 (60%; 15/25 patients) and distal mutations/exons 63–79 (two patients). We summarize that small sample sizes in genetic subgroups underpowered this study, impairing meaningful statistical analysis. A larger sample would possibly show findings similar to those of other researchers [4-8,11,13,14,17-21,38,39].
The main limitations of this study were the small sample size, which impaired statistical relevance of some results, and limited data about MMSE in childhood. It's possible that scientific disinterest in exploring MMSE in DMD patients is because it is not accurate to detect subtle cognitive problems in early ages.
In conclusion, we provide data regarding the MMSE as a screening test for ID in boys with DMD from the age 9 years and up. Scores equal to, or under, 21 showed 78% accuracy, 82% sensitivity, and 74% specificity for ID. Given that normal children achieve 24 points in the MMSE at 6 years of age, and DMD patients without ID surpass this cutoff only after 9 to 10 years of age, it is evident that learning disabilities affect all boys with DMD, to a greater or lesser degree. The MMSE adds standard clinical evaluation, and provides a quantitative measure of mental function in DMD patients that can help in making decisions about pedagogical and academic interventions in literacy, in underprivileged public health systems. Subtests of the MMSE with better discriminatory power (for orientation, attention and calculation) can help educators, teachers, and families develop simple activities or games that enhance such mental skills. Considering that neuropsychological batteries are unavailable in many developing countries, cognitive screening tests like the MMSE may be the best options for strengthening clinical diagnoses, and help families, associations, schools and health professionals understand the prevalent neurocognitive handicaps of boys with DMD.
Notes
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: FN and APQCA. Data curation: FN, MB, and HFG. Formal analysis: FN. Funding acquisition: FN. Methodology: FN and APQCA. Project administration: FN and APQCA. Visualization: FN, APQCA, and MGR. Writing original draft: FN. Writing-review & editing: FN, APQCA, and MGR.
Acknowledgements
We would like to thank professor Ronir Raggio and his assistent Jéssica Pronestino for their statistical support on this study.