Introduction
Autism spectrum disorder (ASD) encompasses a range of neurodevelopmental disorders characterised by challenges in social interaction and communication, restricted interests, repetitive and stereotypical behaviours, and sensory processing issues that typically appear in early childhood [1]. The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, published by the American Psychiatric Association, classifies childhood autism, pervasive developmental disorder not otherwise specified, and Asperger's syndrome under the umbrella of ASD [2]. Genetic factors are believed to contribute to 10% to 20% of ASD cases [3]. Potential environmental factors include advanced parental age, birth by caesarean section, exposure to lead, maternal obesity, hypertension, air pollution, and diabetes [4-8].
Vitamin D is widely recognised for its immunomodulatory properties. The active form of vitamin D, calcitriol, can bind to vitamin D receptors (VDRs) and modify gene transcription. These VDRs are expressed by all immune cells in the human body, enabling vitamin D to carry out a range of functions [9]. It is estimated that 30% of the global population is deficient in vitamin D, while 60% have suboptimal levels [10]. Recent discoveries have highlighted the importance of vitamin D in the development of the foetal and early postnatal brain, beyond its established role in regulating calcium and phosphorus levels. An increasing amount of evidence indicates that vitamin D is implicated in the pathogenesis of ASD, and that vitamin D deficiency may be a contributing factor to ASD [11]. Concurrently, some studies have demonstrated that vitamin D can ameliorate the core symptoms in children with ASD [12]. This review summarises the relationship between vitamin D levels and ASD, explores the potential mechanisms by which vitamin D may be involved in ASD, and discusses the impact of vitamin D supplementation on ASD.
Autism Spectrum Disorder
1. Epidemiology, etiology, and pathogenesis of autism spectrum disorder
ASD was once considered a rare condition; however, its prevalence has surged in recent decades across various countries [13]. The World Health Organisation reports a global prevalence of ASD at 0.76%, but this figure represents about 16% of the global child population [14]. The Centres for Disease Control and Prevention indicate that, in the United States, the prevalence of autism among 8-year-old children was one in 54 in 2016, with a male-to-female ratio of 4.3:1 [15]. Although there are no national data on the ASD epidemic in China, a multicentre study suggests that the prevalence of ASD among children aged 6 to 10 years is approximately 1% in China, which points to an upward trend [16]. ASD impacts children across all racial, ethnic, and socioeconomic backgrounds, yet the rates of diagnosis vary significantly. Caucasian children are diagnosed with ASD more frequently than black or Hispanic children [17]. Studies have also found that ASD is more prevalent in urban areas compared to rural regions. This is attributed to factors such as rainy and cloudy weather, reduced exposure to ultraviolet B (UVB) rays, and higher levels of air pollution, all of which diminish ultraviolet radiation at the Earth's surface and, consequently, vitamin D synthesis in the skin [18-20]. These findings lend support to the aetiological theory that a deficiency in vitamin D may contribute to the development of ASD.
ASD is a neurobiological disorder shaped by a combination of genetic and environmental factors that influence brain development [21]. Although there have been relatively few neuropathological studies, findings have identified abnormalities in the limbic system, differences in cerebellar structure and connectivity, and alterations in the cortical areas of the frontal and temporal lobes, along with other subtle malformations [22-24]. A small-scale exploratory study examining the neocortical architecture of young children indicated a focal disruption in the cortical laminar structure in the majority of participants, suggesting problems with the formation of cortical layers and neuronal differentiation [25]. Brain overgrowth, characterised by both an increase in cortical size and a rise in extra-axial fluid, has been observed in children with ASD. This phenomenon is an area of ongoing research, aimed at improving our understanding of its origins and investigating its potential as a biomarker [26,27].
Siblings of individuals with ASD exhibit an increased risk of receiving a diagnosis than the general population, and identical twins demonstrate a significantly higher—but not guaranteed—rate of concordance for an ASD diagnosis [28-30]. ASD is associated with genes that produce proteins crucial for neuronal synapses or those involved in neurons’ activity-dependent changes, such as transcription factors [28,31]. Epigenetic alterations, including DNA methylation and histone acetylation, as well as disruptions in transcription and splicing, may also contribute to the condition [28,32-34]. ASD is one of the most genetically diverse neuropsychiatric disorders, with rare de novo and inherited variants identified in over 700 genes [35]. The manifestation of genetic predispositions in ASD exhibits a broad spectrum [36]. Environmental factors occurring before, during, and after birth may also modulate the genetic susceptibility in some individuals [37]. Increased risks of having a child with ASD have been associated with both older maternal and paternal ages [38]. While a maternal history of autoimmune diseases, such as diabetes, thyroid disorders, or psoriasis, has been suggested as a potential risk factor, research findings have been inconsistent [39,40]. Recent studies have highlighted maternal infection or immune activation during pregnancy as another area of interest, potentially representing a risk factor [41-43]. The risk for ASD has been associated with both shorter and longer intervals between pregnancies [44]. Additionally, premature infants face a heightened risk for ASD and other neurodevelopmental disorders [45]. Obstetric complications such as preeclampsia, preterm birth, caesarean delivery, low birth weight, uterine bleeding, and low Apgar scores have been identified as some of the more consistently associated factors with autism in previous epidemiological reviews [46].
2. Vitamin D: production and metabolism
Vitamin D is a fat-soluble vitamin encompassing a group of steroid-like substances, including ergocalciferol (D2) and cholecalciferol (D3) [47]. This essential nutrient is synthesised in the skin when 7-dehydrocholesterol interacts with UVB radiation [48]. Subsequently, it undergoes two hydroxylation processes in the liver and kidneys to form 1,25(OH)D and then 1,25(OH)2D3, which activates VDRs to elicit a biological response. Due to the strict regulation of 1,25(OH)2D3 synthesis, serum 25-(OH)D is considered the most reliable indicator of vitamin D status. Traditionally, vitamin D has been recognised for its role in regulating calcium and phosphorus metabolism, which is vital for bone growth and development [49]. However, recent studies have revealed that the enzyme crucial for vitamin D synthesis, 1α-hydroxylase, along with VDRs, is prevalent in brain tissue, indicating that vitamin D is also crucial for brain development [50]. Vitamin D contributes to brain development and function by modulating synaptic plasticity, influencing the dopaminergic system, and reducing oxidative stress [51]. Furthermore, research suggests that vitamin D3 may enhance the formation of regulatory T-cells, thereby preventing excessive immune responses and autoimmune conditions [52].
Association of Vitamin D Levels with Autism Spectrum Disorder
Increasingly many researchers are examining changes in serum vitamin D levels in ASD children. Numerous studies on the vitamin D status of children and adolescents with ASD from multiple regions and backgrounds have found that ASD children and adolescents had lower vitamin D levels [53-59]. Studies have revealed that vitamin D concentrations in children with ASD are not only lower than those in control groups, but also that there is a significant negative correlation between vitamin D levels and total scores on various assessment tools, including the Social Responsiveness Scale (SRS), Autism Treatment Evaluation Checklist (ATEC), ATEC's social affect domain, Autism Behaviour Checklist (ABC), the behavioural affect domain, and the Childhood Autism Rating Scale (CARS). This correlation suggests that lower vitamin D levels are associated with increased severity of autism symptoms [60,61]. Furthermore, a meta-analysis has confirmed that children and adolescents with ASD have significantly lower levels of vitamin D than participants in control groups [12].
There is evidence suggesting a link between maternal 25-(OH)D levels during pregnancy and neurodevelopmental outcomes in children. Specifically, children whose mothers had low prenatal 25-(OH)D levels (less than 20 ng/mL) exhibited more symptoms associated with ASD, faced greater cognitive challenges, and demonstrated poorer social skills by the age of 5 [62]. One study found that mothers with ASD had significantly lower maternal serum concentrations of 25-(OH)D than mothers without ASD, with 55.9% and 29.4% of them experiencing vitamin D deficiency, respectively [63]. Furthermore, reduced serum levels of 25-(OH)D in the first trimester, as well as low maternal vitamin D levels in the second trimester and at birth, have been associated with a significantly increased risk of ASD in offspring [64]. Additionally, it has been shown that low vitamin D levels during pregnancy and limited exposure to solar UVB radiation may elevate the risk of ASD [65]. Higher prenatal 25-(OH)D levels positively affect cognitive development in offspring, and 25-(OH)D levels in early pregnancy may exert a stronger impact on neurodevelopment than levels later in pregnancy [49].
Mechanism of Vitamin D’s Involvement in Autism Spectrum Disorder
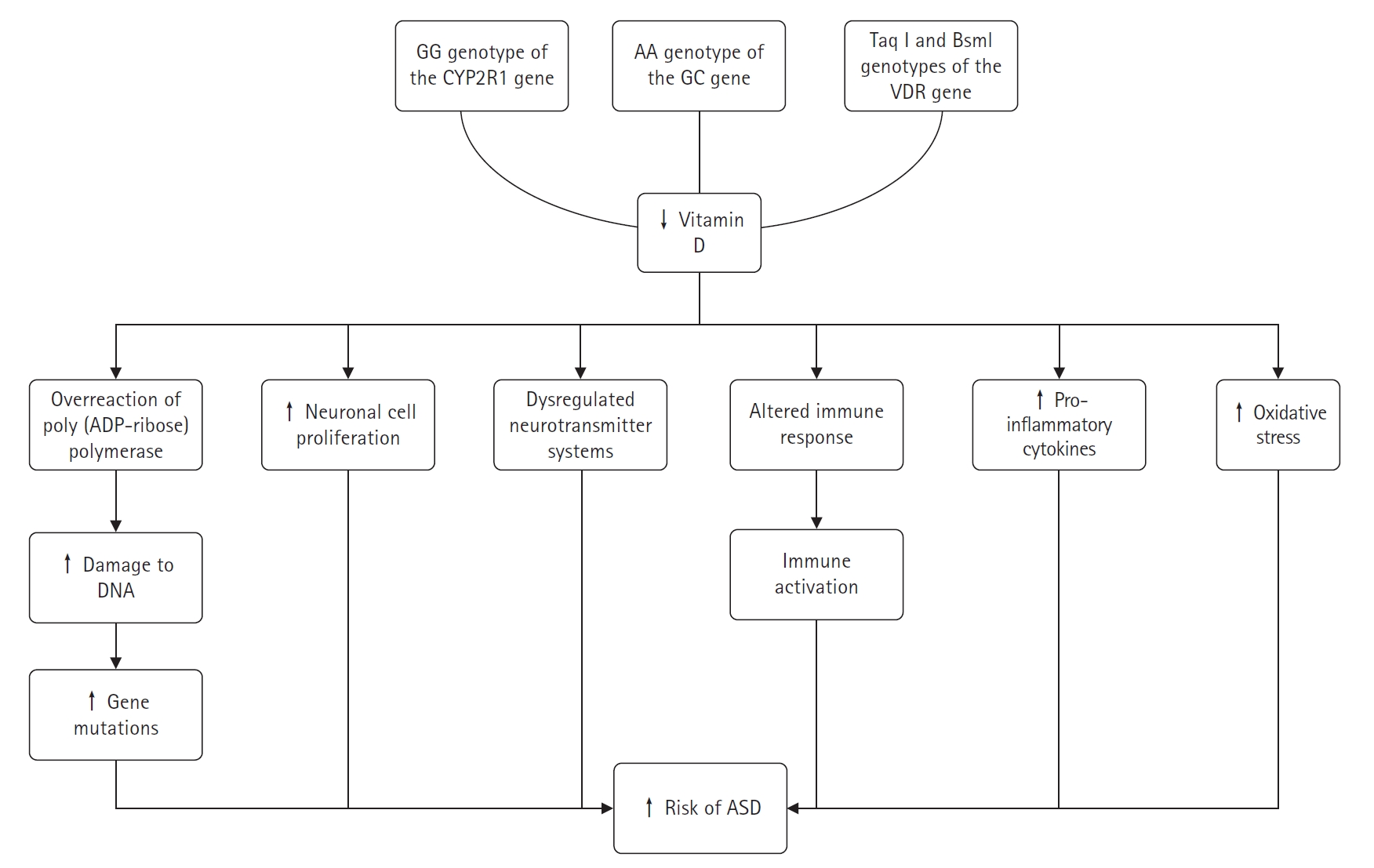
It was found that children with the GG genotype of the cytochrome P450 family 2 subfamily R member 1 (CYP2R1) gene (encoding an enzyme that catalyses the conversion of vitamin D to 25-(OH)D), the AA genotype of the GC gene (encoding a vitamin D-binding protein), and the paternal Taq l and Bsml genotypes of the VDR gene had an increased risk of ASD, emphasising the possible aetiological role of low vitamin D concentrations in ASD [66]. Recent genetic studies on ASD have identified numerous neonatal mutations in affected children [25]. Vitamin D is capable of DNA repair and maintenance through several mechanisms. To date, over five vitamin D-dependent genes have been identified that encode proteins involved in the permanent repair of DNA mutations [67]. Vitamin D has the ability to repair and maintain DNA through a variety of mechanisms. Low vitamin D levels can lead to an overactivation of the DNA repair enzyme poly(adenosine diphosphate ribose) polymerase, which may inadvertently damage adjacent DNA. Daily supplementation with low doses of vitamin D3 has been shown to prevent gene mutations, enhance apoptosis, and increase Bax levels [68]. Research has established that several proteins closely associated with vitamin D, such as growth arrest and DNA-damage-inducible alpha, RAD23 homolog B, and poly(adenosine diphosphate ribose), play roles in DNA damage repair [25,67-69]. Consequently, vitamin D deficiency may contribute to gene mutations in children with ASD.
When vitamin D levels are insufficient, neuronal cells may proliferate excessively, leading to increased brain growth during early development stages, which could be associated with the onset of ASD [70,71]. In neuroanatomy, animal models of developmental vitamin D deficiency have successfully replicated phenotypes associated with ASD [72]. Vitamin D-related neurotransmitters, including 5-hydroxytryptamine, oxytocin, serotonin, dopamine, and γ-aminobutyric acid, are known to regulate learning, memory, and emotions [73-75]. Dysregulation of neurotransmitter systems, such as the oxytocinergic, dopaminergic, and serotonergic systems, is thought to contribute to ASD. These systems are crucial for brain maturation, neurotransmission, behaviour, and cortical organisation [74]. Rodent studies have shown that vitamin D administration can increase gamma-aminobutyric acid (GABA) production in brain regions like the hippocampus, anterior cingulate cortex, and prefrontal cortex [73]. Individuals with ASD have been found to have lower plasma oxytocin levels and abnormal serotonin concentrations in the brain and peripheral tissues [74]. Brain dopamine transporter binding is significantly higher in ASD patients compared to healthy controls, while brain serotonin transporter binding is significantly lower in high-functioning adults with ASD [76]. There is evidence of increased peripheral blood 5-hydroxytryptamine (serotonin) and decreased brain concentrations in individuals with ASD [74].
Immune activation is considered a risk factor for ASD. A deficiency in vitamin D may alter the immune responses of ASD patients and could prevent behavioural issues related to immune activation [76]. Autoimmune markers, such as anti-ganglioside M1 antibodies, anti-nucleosome-specific antibodies, anti-nuclear antibodies, and anti-myelin basic protein autoantibodies, are more prevalent in ASD patients, with their levels positively correlating with ASD severity [64]. Mostafa and Al-Ayadhi [77] found that anti-myelin-associated glycoprotein (anti-MAG) levels were higher in 70% of children with ASD, and there was a significant negative correlation between serum 25-(OH)D levels and anti-MAG levels. This suggests that vitamin D deficiency in some children with ASD may contribute to elevated anti-MAG levels, which could play a role in brain damage associated with ASD. These findings highlight the importance of vitamin D in the development of autoantibodies and the pathophysiology of ASD. According to recent research, ASD is an inflammatory disease [54,55]. Vitamin D is known to have an immunomodulatory effect, enhancing protective immune responses while reducing inflammatory ones [78]. The anti-inflammatory effects of vitamin D on the brain include reducing neurotoxicity, oxidative-induced neuroinflammation, and harmful inflammatory cytokines. Abnormal immune function in people with ASD, such as elevated inflammatory cytokine levels, is similar to that seen in vitamin D deficiency [19]. Pro-inflammatory cytokines like interferon-γ, tumour necrosis factor-α (TNF-α), and interleukin-6 (IL-6) are found in higher concentrations in children with ASD and are associated with cognitive impairment [79,80]. Vitamin D metabolites have been shown to decrease the release of TNF-α and IL-6, increase the expression of anti-inflammatory cytokines like interleukin-10 (IL-10) from activated B-cells, and promote a more tolerogenic state in dendritic cells. The activation of calcitriol leads to lower production of inflammatory cytokines, thereby protecting brain tissue [81].
Vitamin D supplementation is thought to reduce oxidative stress and play a protective role in the brain. Several lines of evidence suggest that oxidative stress and mitochondrial dysfunction are common in ASD [82]. Children with ASD have higher levels of oxidised glutathione in their plasma, which causes a corresponding rise in oxidative stress [83]. Vitamin D is an antioxidant that can increase glutathione levels, decrease glial cell activation, inhibit nitric oxide synthase synthesis, and attenuate neuroinflammation; thus, it plays an important role in neuromodulation and neuroprotection [84].
Neuroanatomical defects in vitamin D-deficient mice include increased brain volume and lateral ventricle size, aberrant brain calcium signalling, and dysfunctional mitochondria. These mice also demonstrate an increased vulnerability to oxidative stress, alterations in dopamine and serotonin signalling that lead to changes in neurotransmission, and a distinctly atypical immune response associated with a higher risk of autoimmune diseases and chronic inflammatory conditions [72]. The behaviour of young children with autism shows similarities to that of vitamin D-deficient animals [85]. Vitamin D supplementation may influence animal models of ASD, and the timing of vitamin D deficiency may determine the presence or absence of ASD-related symptoms in rodent studies [54,86,87]. Fig. 1 summarizes the complex role of vitamin D in the development of ASD.
Effect of Vitamin D Supplementation on Autism Spectrum Disorder
A prospective study that administered vitamin D to pregnant women who already had children with autism found that only 5% of their new-borns were diagnosed with autism, a figure notably lower than the rates of 20% or higher reported in existing literature [86,88]. However, some researchers caution against drawing firm conclusions from these findings, as the study lacked a control group and involved a relatively small sample of pregnant women with varying lengths of vitamin D supplementation. They contend that the current evidence does not substantiate the claim that vitamin D supplementation during pregnancy can prevent the onset of ASD [89]. In a 2014 study, a 32-month-old boy with ASD and a deficiency in vitamin D received a daily oral dose of 400 IU of vitamin D3 and a monthly intramuscular injection of 150,000 IU of vitamin D3 for 2 months. This treatment led to temporary improvements in the core symptoms of ASD [90]. A case-control study published in 2015 reported that after 6 months of vitamin D supplementation, participants showed improvements in scores on the CARS, the Vineland Adaptive Behaviour Scale, and the ATEC. Although the group that received vitamin D supplements exhibited slight improvements in ASD symptoms, the differences between the supplemented and non-supplemented groups were not statistically significant [91]. Another study indicated that 37 children with ASD and low vitamin D levels (25-(OH)D <75 nm/L) who received vitamin D supplements for 3 months experienced significant enhancements in ASD symptoms, as measured by the ABC and CARS scores [92]. The latest randomised controlled trials and meta-analyses of vitamin D for the treatment of ASD have also shown that vitamin D can improve the core symptoms of ASD [93,94].
Conclusion
The high incidence of ASD has turned it into a pressing social issue, yet the etiology of the disorder remains elusive. While ASD is believed to be influenced by a combination of genetic and environmental factors, existing research has not satisfactorily accounted for the disorder's epidemiological traits, and pharmacological interventions have yet to prove effective. Consequently, exploring the origins and development of ASD from a novel angle is crucial for devising ground-breaking treatment strategies. There is evidence to suggest that insufficient vitamin D levels during pregnancy, after birth, and in early childhood may be associated with neurodevelopmental disorders, including ASD. Certain studies indicate that vitamin D supplementation in vitamin D-deficient children with ASD can ameliorate their fundamental symptoms. To fully comprehend the connection between vitamin D and ASD, extensive research is required. Delving deeper into this relationship could pave the way for a straightforward, cost-effective, and safe new approach to treating and preventing ASD.